Rebaz Ali, Omar H Ghalib Hawramy, Fahmi H Kakamad, Dlshad Hamasaeed, Soran H Tahir, Deari A Ismaeil, Bahra A Awalmohammed, Hemn H Kaka Ali, Bruj Jamil Mohammed, Hiwa O Abdullah, Berun A Abdalla
{"title":"胃食管腺癌转移至胸壁:1例报告及文献回顾。","authors":"Rebaz Ali, Omar H Ghalib Hawramy, Fahmi H Kakamad, Dlshad Hamasaeed, Soran H Tahir, Deari A Ismaeil, Bahra A Awalmohammed, Hemn H Kaka Ali, Bruj Jamil Mohammed, Hiwa O Abdullah, Berun A Abdalla","doi":"10.3892/mi.2023.91","DOIUrl":null,"url":null,"abstract":"<p><p>Subcutaneous metastasis from esophageal cancer (EC), particularly to the chest wall, is a very rare phenomenon. The present study describes a case of gastroesophageal adenocarcinoma that metastasized to the chest wall, invading the fourth anterior rib. A 70-year-old female presented with acute chest pain 4 months after undergoing Ivor-Lewis esophagectomy for gastroesophageal adenocarcinoma. A chest ultrasound revealed a solid hypoechoic mass on the right side of the chest. A contrast-enhanced computed tomography scan of the chest revealed a destructive mass on the right anterior fourth rib (7.5x5 cm). Fine needle aspiration revealed a metastatic moderately differentiated adenocarcinoma to the chest wall. Fluorodeoxyglucose (FDG)-positron emission tomography/computed tomography revealed a large FDG avid deposit on the right side of the chest wall. Under general anesthesia, a right-side anterior chest incision was made and the second, third and fourth ribs were resected with overlying soft tissues, including the pectoralis muscle and overlying skin. The histopathological examination confirmed a metastasized gastroesophageal adenocarcinoma to the chest wall. There are two common assumptions regarding chest wall metastasis from EC. The first one states that this metastasis can occur due to the implantation of the carcinoma during tumor resection. The latter supports the notion of tumor cell dissemination along the esophageal lymphatic and hematogenous systems. Chest wall metastasis from EC invading ribs is an extremely rare incident. However, its likelihood of occurrence should not be neglected following primary cancer treatment.</p>","PeriodicalId":74161,"journal":{"name":"Medicine international","volume":"3 3","pages":"31"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10288431/pdf/","citationCount":"0","resultStr":"{\"title\":\"Gastroesophageal adenocarcinoma metastasizing to the chest wall: A case report and mini‑review of the literature.\",\"authors\":\"Rebaz Ali, Omar H Ghalib Hawramy, Fahmi H Kakamad, Dlshad Hamasaeed, Soran H Tahir, Deari A Ismaeil, Bahra A Awalmohammed, Hemn H Kaka Ali, Bruj Jamil Mohammed, Hiwa O Abdullah, Berun A Abdalla\",\"doi\":\"10.3892/mi.2023.91\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Subcutaneous metastasis from esophageal cancer (EC), particularly to the chest wall, is a very rare phenomenon. The present study describes a case of gastroesophageal adenocarcinoma that metastasized to the chest wall, invading the fourth anterior rib. A 70-year-old female presented with acute chest pain 4 months after undergoing Ivor-Lewis esophagectomy for gastroesophageal adenocarcinoma. A chest ultrasound revealed a solid hypoechoic mass on the right side of the chest. A contrast-enhanced computed tomography scan of the chest revealed a destructive mass on the right anterior fourth rib (7.5x5 cm). Fine needle aspiration revealed a metastatic moderately differentiated adenocarcinoma to the chest wall. Fluorodeoxyglucose (FDG)-positron emission tomography/computed tomography revealed a large FDG avid deposit on the right side of the chest wall. Under general anesthesia, a right-side anterior chest incision was made and the second, third and fourth ribs were resected with overlying soft tissues, including the pectoralis muscle and overlying skin. The histopathological examination confirmed a metastasized gastroesophageal adenocarcinoma to the chest wall. There are two common assumptions regarding chest wall metastasis from EC. The first one states that this metastasis can occur due to the implantation of the carcinoma during tumor resection. The latter supports the notion of tumor cell dissemination along the esophageal lymphatic and hematogenous systems. Chest wall metastasis from EC invading ribs is an extremely rare incident. However, its likelihood of occurrence should not be neglected following primary cancer treatment.</p>\",\"PeriodicalId\":74161,\"journal\":{\"name\":\"Medicine international\",\"volume\":\"3 3\",\"pages\":\"31\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10288431/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medicine international\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3892/mi.2023.91\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medicine international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3892/mi.2023.91","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Gastroesophageal adenocarcinoma metastasizing to the chest wall: A case report and mini‑review of the literature.
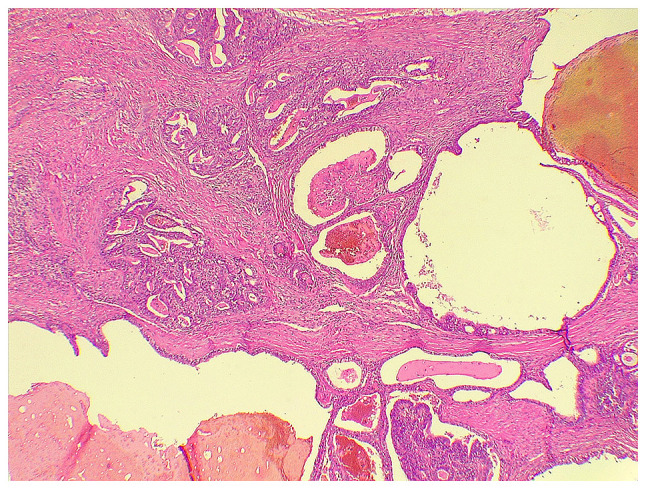
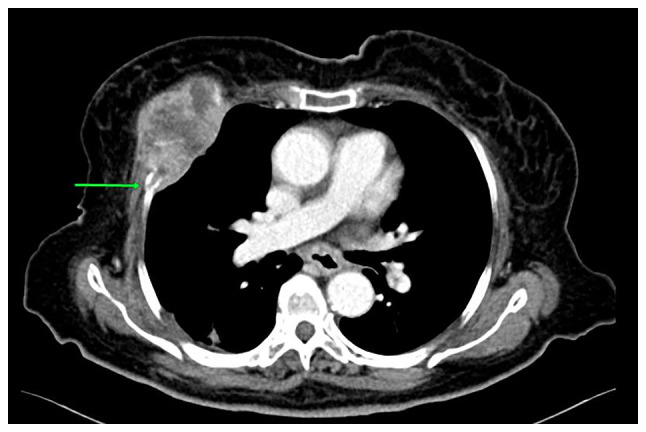
Subcutaneous metastasis from esophageal cancer (EC), particularly to the chest wall, is a very rare phenomenon. The present study describes a case of gastroesophageal adenocarcinoma that metastasized to the chest wall, invading the fourth anterior rib. A 70-year-old female presented with acute chest pain 4 months after undergoing Ivor-Lewis esophagectomy for gastroesophageal adenocarcinoma. A chest ultrasound revealed a solid hypoechoic mass on the right side of the chest. A contrast-enhanced computed tomography scan of the chest revealed a destructive mass on the right anterior fourth rib (7.5x5 cm). Fine needle aspiration revealed a metastatic moderately differentiated adenocarcinoma to the chest wall. Fluorodeoxyglucose (FDG)-positron emission tomography/computed tomography revealed a large FDG avid deposit on the right side of the chest wall. Under general anesthesia, a right-side anterior chest incision was made and the second, third and fourth ribs were resected with overlying soft tissues, including the pectoralis muscle and overlying skin. The histopathological examination confirmed a metastasized gastroesophageal adenocarcinoma to the chest wall. There are two common assumptions regarding chest wall metastasis from EC. The first one states that this metastasis can occur due to the implantation of the carcinoma during tumor resection. The latter supports the notion of tumor cell dissemination along the esophageal lymphatic and hematogenous systems. Chest wall metastasis from EC invading ribs is an extremely rare incident. However, its likelihood of occurrence should not be neglected following primary cancer treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


