{"title":"外周诱发的运动障碍:最新进展。","authors":"Abhishek Lenka, Joseph Jankovic","doi":"10.5334/tohm.758","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Peripherally-induced movement disorders (PIMD) should be considered when involuntary or abnormal movements emerge shortly after an injury to a body part. A close topographic and temporal association between peripheral injury and onset of the movement disorders is crucial to diagnosing PIMD. PIMD is under-recognized and often misdiagnosed as functional movement disorder, although both may co-exist. Given the considerable diagnostic, therapeutic, and psychosocial-legal challenges associated with PIMD, it is crucial to update the clinical and scientific information about this important movement disorder.</p><p><strong>Methods: </strong>A comprehensive PubMed search through a broad range of keywords and combinations was performed in February 2023 to identify relevant articles for this narrative review.</p><p><strong>Results: </strong>The spectrum of the phenomenology of PIMD is broad and it encompasses both hyperkinetic and hypokinetic movements. Hemifacial spasm is probably the most common PIMD. Others include dystonia, tremor, parkinsonism, myoclonus, painful leg moving toe syndrome, tics, polyminimyoclonus, and amputation stump dyskinesia. We also highlight conditions such as neuropathic tremor, pseudoathetosis, and <i>MYBPC1</i>-associated myogenic tremor as examples of PIMD.</p><p><strong>Discussion: </strong>There is considerable heterogeneity among PIMD in terms of severity and nature of injury, natural course, association with pain, and response to treatment. As some patients may have co-existing functional movement disorder, neurologists should be able to differentiate the two disorders. While the exact pathophysiology remains elusive, aberrant central sensitization after peripheral stimuli and maladaptive plasticity in the sensorimotor cortex, on a background of genetic (two-hit hypothesis) or other predisposition, seem to play a role in the pathogenesis of PIMD.</p>","PeriodicalId":23317,"journal":{"name":"Tremor and Other Hyperkinetic Movements","volume":null,"pages":null},"PeriodicalIF":2.5000,"publicationDate":"2023-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10064913/pdf/","citationCount":"0","resultStr":"{\"title\":\"Peripherally-induced Movement Disorders: An Update.\",\"authors\":\"Abhishek Lenka, Joseph Jankovic\",\"doi\":\"10.5334/tohm.758\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Peripherally-induced movement disorders (PIMD) should be considered when involuntary or abnormal movements emerge shortly after an injury to a body part. A close topographic and temporal association between peripheral injury and onset of the movement disorders is crucial to diagnosing PIMD. PIMD is under-recognized and often misdiagnosed as functional movement disorder, although both may co-exist. Given the considerable diagnostic, therapeutic, and psychosocial-legal challenges associated with PIMD, it is crucial to update the clinical and scientific information about this important movement disorder.</p><p><strong>Methods: </strong>A comprehensive PubMed search through a broad range of keywords and combinations was performed in February 2023 to identify relevant articles for this narrative review.</p><p><strong>Results: </strong>The spectrum of the phenomenology of PIMD is broad and it encompasses both hyperkinetic and hypokinetic movements. Hemifacial spasm is probably the most common PIMD. Others include dystonia, tremor, parkinsonism, myoclonus, painful leg moving toe syndrome, tics, polyminimyoclonus, and amputation stump dyskinesia. We also highlight conditions such as neuropathic tremor, pseudoathetosis, and <i>MYBPC1</i>-associated myogenic tremor as examples of PIMD.</p><p><strong>Discussion: </strong>There is considerable heterogeneity among PIMD in terms of severity and nature of injury, natural course, association with pain, and response to treatment. As some patients may have co-existing functional movement disorder, neurologists should be able to differentiate the two disorders. While the exact pathophysiology remains elusive, aberrant central sensitization after peripheral stimuli and maladaptive plasticity in the sensorimotor cortex, on a background of genetic (two-hit hypothesis) or other predisposition, seem to play a role in the pathogenesis of PIMD.</p>\",\"PeriodicalId\":23317,\"journal\":{\"name\":\"Tremor and Other Hyperkinetic Movements\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-03-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10064913/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tremor and Other Hyperkinetic Movements\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5334/tohm.758\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tremor and Other Hyperkinetic Movements","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5334/tohm.758","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Peripherally-induced Movement Disorders: An Update.
Background: Peripherally-induced movement disorders (PIMD) should be considered when involuntary or abnormal movements emerge shortly after an injury to a body part. A close topographic and temporal association between peripheral injury and onset of the movement disorders is crucial to diagnosing PIMD. PIMD is under-recognized and often misdiagnosed as functional movement disorder, although both may co-exist. Given the considerable diagnostic, therapeutic, and psychosocial-legal challenges associated with PIMD, it is crucial to update the clinical and scientific information about this important movement disorder.
Methods: A comprehensive PubMed search through a broad range of keywords and combinations was performed in February 2023 to identify relevant articles for this narrative review.
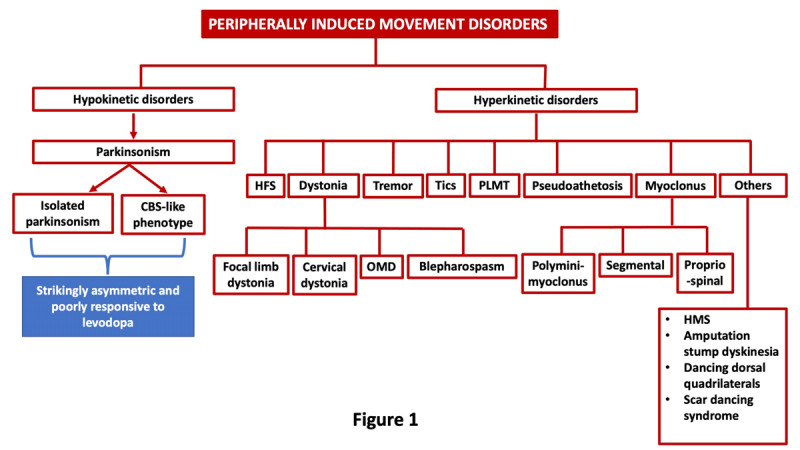
Results: The spectrum of the phenomenology of PIMD is broad and it encompasses both hyperkinetic and hypokinetic movements. Hemifacial spasm is probably the most common PIMD. Others include dystonia, tremor, parkinsonism, myoclonus, painful leg moving toe syndrome, tics, polyminimyoclonus, and amputation stump dyskinesia. We also highlight conditions such as neuropathic tremor, pseudoathetosis, and MYBPC1-associated myogenic tremor as examples of PIMD.
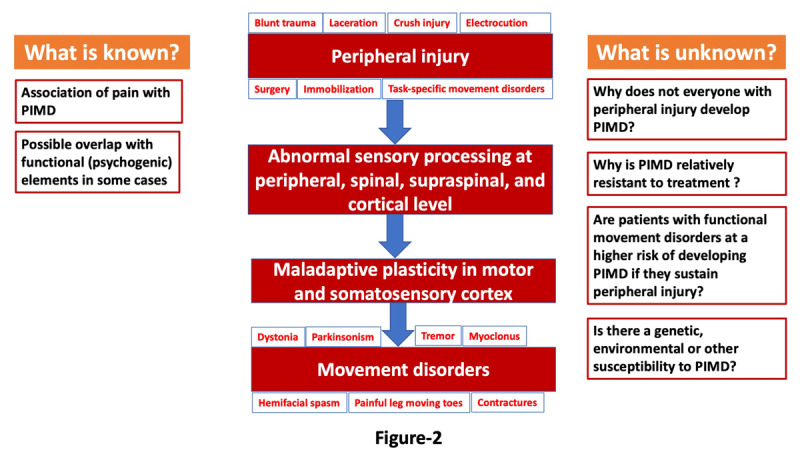
Discussion: There is considerable heterogeneity among PIMD in terms of severity and nature of injury, natural course, association with pain, and response to treatment. As some patients may have co-existing functional movement disorder, neurologists should be able to differentiate the two disorders. While the exact pathophysiology remains elusive, aberrant central sensitization after peripheral stimuli and maladaptive plasticity in the sensorimotor cortex, on a background of genetic (two-hit hypothesis) or other predisposition, seem to play a role in the pathogenesis of PIMD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


