Calvin Ke, Emaad Mohammad, Juliana C N Chan, Alice P S Kong, Fok-Han Leung, Baiju R Shah, Douglas Lee, Andrea O Luk, Ronald C W Ma, Elaine Chow, Xiaolin Wei
{"title":"安大略省和香港以团队为基础的糖尿病护理:比较回顾。","authors":"Calvin Ke, Emaad Mohammad, Juliana C N Chan, Alice P S Kong, Fok-Han Leung, Baiju R Shah, Douglas Lee, Andrea O Luk, Ronald C W Ma, Elaine Chow, Xiaolin Wei","doi":"10.1007/s11892-023-01508-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of review: </strong>There are gaps in implementing and accessing team-based diabetes care. We reviewed and compared how team-based diabetes care was implemented in the primary care contexts of Ontario and Hong Kong.</p><p><strong>Recent findings: </strong>Ontario's Diabetes Education Programs (DEPs) were scaled-up incrementally. Hong Kong's Multidisciplinary Risk Assessment and Management Program for Diabetes Mellitus (RAMP-DM) evolved from a research-driven quality improvement program. Each jurisdiction had a mixture of non-team and team-based primary care with variable accessibility. Referral procedures, follow-up processes, and financing models varied. DEPs used a flexible approach, while the RAMP-DM used structured assessment for quality assurance. Each approach depended on adequate infrastructure, processes, and staff. Diabetes care is most accessible and functional when integrated team-based services are automatically initiated upon diabetes diagnosis within a strong primary care system, ideally linked to a register with supports including specialist care. Structured assessment and risk stratification are the basis of a well-studied, evidence-based approach for achieving the standards of team-based diabetes care, although flexibility in care delivery may be needed to meet the unique needs of some individuals. Policymakers and funders should ensure investment in skilled health professionals, infrastructure, and processes to improve care quality.</p>","PeriodicalId":10898,"journal":{"name":"Current Diabetes Reports","volume":"23 7","pages":"135-146"},"PeriodicalIF":6.4000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10091345/pdf/","citationCount":"0","resultStr":"{\"title\":\"Team-Based Diabetes Care in Ontario and Hong Kong: a Comparative Review.\",\"authors\":\"Calvin Ke, Emaad Mohammad, Juliana C N Chan, Alice P S Kong, Fok-Han Leung, Baiju R Shah, Douglas Lee, Andrea O Luk, Ronald C W Ma, Elaine Chow, Xiaolin Wei\",\"doi\":\"10.1007/s11892-023-01508-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose of review: </strong>There are gaps in implementing and accessing team-based diabetes care. We reviewed and compared how team-based diabetes care was implemented in the primary care contexts of Ontario and Hong Kong.</p><p><strong>Recent findings: </strong>Ontario's Diabetes Education Programs (DEPs) were scaled-up incrementally. Hong Kong's Multidisciplinary Risk Assessment and Management Program for Diabetes Mellitus (RAMP-DM) evolved from a research-driven quality improvement program. Each jurisdiction had a mixture of non-team and team-based primary care with variable accessibility. Referral procedures, follow-up processes, and financing models varied. DEPs used a flexible approach, while the RAMP-DM used structured assessment for quality assurance. Each approach depended on adequate infrastructure, processes, and staff. Diabetes care is most accessible and functional when integrated team-based services are automatically initiated upon diabetes diagnosis within a strong primary care system, ideally linked to a register with supports including specialist care. Structured assessment and risk stratification are the basis of a well-studied, evidence-based approach for achieving the standards of team-based diabetes care, although flexibility in care delivery may be needed to meet the unique needs of some individuals. Policymakers and funders should ensure investment in skilled health professionals, infrastructure, and processes to improve care quality.</p>\",\"PeriodicalId\":10898,\"journal\":{\"name\":\"Current Diabetes Reports\",\"volume\":\"23 7\",\"pages\":\"135-146\"},\"PeriodicalIF\":6.4000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10091345/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Diabetes Reports\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11892-023-01508-0\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Diabetes Reports","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11892-023-01508-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
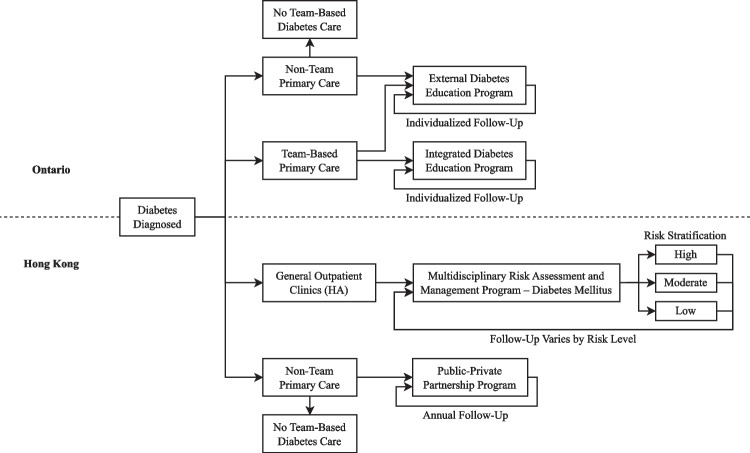
Team-Based Diabetes Care in Ontario and Hong Kong: a Comparative Review.
Purpose of review: There are gaps in implementing and accessing team-based diabetes care. We reviewed and compared how team-based diabetes care was implemented in the primary care contexts of Ontario and Hong Kong.
Recent findings: Ontario's Diabetes Education Programs (DEPs) were scaled-up incrementally. Hong Kong's Multidisciplinary Risk Assessment and Management Program for Diabetes Mellitus (RAMP-DM) evolved from a research-driven quality improvement program. Each jurisdiction had a mixture of non-team and team-based primary care with variable accessibility. Referral procedures, follow-up processes, and financing models varied. DEPs used a flexible approach, while the RAMP-DM used structured assessment for quality assurance. Each approach depended on adequate infrastructure, processes, and staff. Diabetes care is most accessible and functional when integrated team-based services are automatically initiated upon diabetes diagnosis within a strong primary care system, ideally linked to a register with supports including specialist care. Structured assessment and risk stratification are the basis of a well-studied, evidence-based approach for achieving the standards of team-based diabetes care, although flexibility in care delivery may be needed to meet the unique needs of some individuals. Policymakers and funders should ensure investment in skilled health professionals, infrastructure, and processes to improve care quality.
期刊介绍:
The goal of this journal is to publish cutting-edge reviews on subjects pertinent to all aspects of diabetes epidemiology, pathophysiology, and management. We aim to provide incisive, insightful, and balanced contributions from leading experts in each relevant domain that will be of immediate interest to a wide readership of clinicians, basic scientists, and translational investigators.
We accomplish this aim by appointing major authorities to serve as Section Editors in key subject areas across the discipline. Section Editors select topics to be reviewed by leading experts who emphasize recent developments and highlight important papers published over the past year on their topics, in a crisp and readable format. We also provide commentaries from well-known figures in the field, and an Editorial Board of internationally diverse members suggests topics of special interest to their country/region and ensures that topics are current and include emerging research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


