Derek Baughman, Kathryn Baughman, Yalda Jabbarpour, Abdul Waheed
{"title":"远程医疗和办公室医疗在异常BMI筛查和管理方面的可比性。","authors":"Derek Baughman, Kathryn Baughman, Yalda Jabbarpour, Abdul Waheed","doi":"10.1002/osp4.625","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite widespread adoption during COVID-19, there is limited evidence supporting the quality of telemedicine care in managing patients with abnormal BMI.</p><p><strong>Objective: </strong>To evaluate the comparability of telemedicine and in-person (office) quality performance for abnormal body mass index (BMI kg/m2) screening and management in primary care.</p><p><strong>Methods: </strong>This retrospective cohort study measured Healthcare Effectiveness Data and Information Set (HEDIS) quality performance for abnormal BMI screening (patients with BMIs <18.5 or >25 kg/m2 and a qualifying documented follow up plan) across an 8-hospital integrated health system seen via primary care from 4/1/20 - 9/30/21. Encounters were divided into three exposure groups: office (excluding telemedicine), telemedicine (excluding office), and blended telemedicine (office + telemedicine). Demographic stratification compared group composition. Chi squared tests determined statistical differences in quality performance (<i>p</i> = <0.05).</p><p><strong>Results: </strong>Demographics of sub-groups for the 287,387 patients (office: 222,333; telemedicine: 1,556; blended-telemedicine: 63,489) revealed a modest female predominance, majority ages 26-70, mostly White non-Hispanics of low health risk, and the majority BMI representation was overweight, followed closely by class 1 obesity. In both HEDIS specified and HEDIS modified performance, blended-telemedicine performed better than office (12.56%, 95% CI 12.29%-13.01%; 11.16%, 95% CI: 10.85%-11.48%; <i>p</i> < 0.0001); office performed better than telemedicine (4.29%, 95% CI 2.84%-5.54%; 4.79%, 95% CI 3.99%-5.35%; <i>p</i> < 0.0001).</p><p><strong>Conclusion: </strong>Quality performance was highest for blended-telemedicine, followed by office-only, then telemedicine-only. Given the known cost savings, adding telemedicine as a care venue might promote value within health systems without negatively impacting HEDIS performance.</p>","PeriodicalId":19448,"journal":{"name":"Obesity Science & Practice","volume":"9 2","pages":"87-94"},"PeriodicalIF":1.9000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cc/50/OSP4-9-87.PMC10073821.pdf","citationCount":"2","resultStr":"{\"title\":\"Comparable quality performance between telemedicine and office-based care for abnormal BMI screening and management.\",\"authors\":\"Derek Baughman, Kathryn Baughman, Yalda Jabbarpour, Abdul Waheed\",\"doi\":\"10.1002/osp4.625\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Despite widespread adoption during COVID-19, there is limited evidence supporting the quality of telemedicine care in managing patients with abnormal BMI.</p><p><strong>Objective: </strong>To evaluate the comparability of telemedicine and in-person (office) quality performance for abnormal body mass index (BMI kg/m2) screening and management in primary care.</p><p><strong>Methods: </strong>This retrospective cohort study measured Healthcare Effectiveness Data and Information Set (HEDIS) quality performance for abnormal BMI screening (patients with BMIs <18.5 or >25 kg/m2 and a qualifying documented follow up plan) across an 8-hospital integrated health system seen via primary care from 4/1/20 - 9/30/21. Encounters were divided into three exposure groups: office (excluding telemedicine), telemedicine (excluding office), and blended telemedicine (office + telemedicine). Demographic stratification compared group composition. Chi squared tests determined statistical differences in quality performance (<i>p</i> = <0.05).</p><p><strong>Results: </strong>Demographics of sub-groups for the 287,387 patients (office: 222,333; telemedicine: 1,556; blended-telemedicine: 63,489) revealed a modest female predominance, majority ages 26-70, mostly White non-Hispanics of low health risk, and the majority BMI representation was overweight, followed closely by class 1 obesity. In both HEDIS specified and HEDIS modified performance, blended-telemedicine performed better than office (12.56%, 95% CI 12.29%-13.01%; 11.16%, 95% CI: 10.85%-11.48%; <i>p</i> < 0.0001); office performed better than telemedicine (4.29%, 95% CI 2.84%-5.54%; 4.79%, 95% CI 3.99%-5.35%; <i>p</i> < 0.0001).</p><p><strong>Conclusion: </strong>Quality performance was highest for blended-telemedicine, followed by office-only, then telemedicine-only. Given the known cost savings, adding telemedicine as a care venue might promote value within health systems without negatively impacting HEDIS performance.</p>\",\"PeriodicalId\":19448,\"journal\":{\"name\":\"Obesity Science & Practice\",\"volume\":\"9 2\",\"pages\":\"87-94\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cc/50/OSP4-9-87.PMC10073821.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Obesity Science & Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/osp4.625\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Obesity Science & Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/osp4.625","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 2
摘要
背景:尽管在COVID-19期间广泛采用了远程医疗,但支持远程医疗在管理BMI异常患者方面质量的证据有限。目的:评价远程医疗与面对面(办公室)质量表现在初级保健中异常体重指数(BMI kg/m2)筛查和管理方面的可比性。方法:本回顾性队列研究测量了在20年1月4日至21年9月30日期间通过初级保健就诊的8家医院综合卫生系统中异常BMI筛查(BMI为25 kg/m2的患者和合格的随访计划)的医疗保健有效性数据和信息集(HEDIS)质量表现。接触者被分为三个暴露组:办公室(不包括远程医疗)、远程医疗(不包括办公室)和混合远程医疗(办公室+远程医疗)。人口分层比较组组成。卡方检验确定了质量表现的统计学差异(p =结果:287,387例患者的亚组人口统计数据(办公室:222,333;远程医疗:1556;混合远程医疗:63,489)显示适度的女性优势,大多数年龄在26-70岁之间,大多数是非西班牙裔的低健康风险白人,大多数BMI代表超重,紧随其后的是1级肥胖。在HEDIS指定和HEDIS改进的性能中,混合远程医疗优于办公室(12.56%,95% CI 12.29%-13.01%;11.16%, 95% ci: 10.85%-11.48%;结论:混合远程医疗的质量绩效最高,纯办公医疗次之,纯远程医疗次之。鉴于已知的成本节约,增加远程医疗作为护理场所可能会提高卫生系统内的价值,而不会对HEDIS的绩效产生负面影响。
Comparable quality performance between telemedicine and office-based care for abnormal BMI screening and management.
Background: Despite widespread adoption during COVID-19, there is limited evidence supporting the quality of telemedicine care in managing patients with abnormal BMI.
Objective: To evaluate the comparability of telemedicine and in-person (office) quality performance for abnormal body mass index (BMI kg/m2) screening and management in primary care.
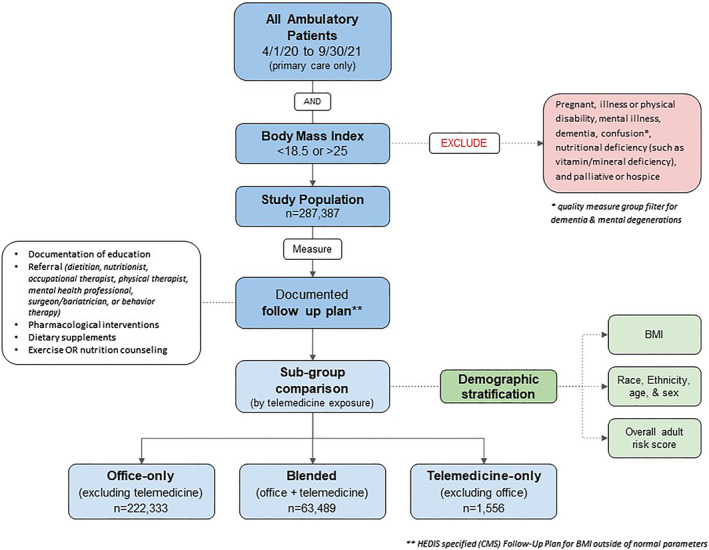
Methods: This retrospective cohort study measured Healthcare Effectiveness Data and Information Set (HEDIS) quality performance for abnormal BMI screening (patients with BMIs <18.5 or >25 kg/m2 and a qualifying documented follow up plan) across an 8-hospital integrated health system seen via primary care from 4/1/20 - 9/30/21. Encounters were divided into three exposure groups: office (excluding telemedicine), telemedicine (excluding office), and blended telemedicine (office + telemedicine). Demographic stratification compared group composition. Chi squared tests determined statistical differences in quality performance (p = <0.05).
Results: Demographics of sub-groups for the 287,387 patients (office: 222,333; telemedicine: 1,556; blended-telemedicine: 63,489) revealed a modest female predominance, majority ages 26-70, mostly White non-Hispanics of low health risk, and the majority BMI representation was overweight, followed closely by class 1 obesity. In both HEDIS specified and HEDIS modified performance, blended-telemedicine performed better than office (12.56%, 95% CI 12.29%-13.01%; 11.16%, 95% CI: 10.85%-11.48%; p < 0.0001); office performed better than telemedicine (4.29%, 95% CI 2.84%-5.54%; 4.79%, 95% CI 3.99%-5.35%; p < 0.0001).
Conclusion: Quality performance was highest for blended-telemedicine, followed by office-only, then telemedicine-only. Given the known cost savings, adding telemedicine as a care venue might promote value within health systems without negatively impacting HEDIS performance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


