{"title":"基于临床变量的肝脂肪变性和肝纤维化预测使用大型国家调查数据库。","authors":"Yanal Alnimer, Touleen Alnimer","doi":"10.1155/2023/1791500","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Vibration-controlled transient elastography (VCTA) and controlled attenuation parameter (CAP) are used more frequently to diagnose liver fibrosis and steatosis among nonalcoholic fatty liver disease patients. However, limited robust data are available on the clinical variables strongly related to these disorders and who needs to be referred for screening.</p><p><strong>Methods: </strong>We used the National Health and Nutritional Examination Survey 2017-2018 database to identify the clinical predictors strongly related to liver steatosis and advanced fibrosis. Baseline comparisons among these groups were made based on widely accepted cutoffs. Linear and logistic regressions were performed to identify the associations between the clinical variables and liver steatosis and fibrosis. We used adaptive lasso regression, gradient-boosted model, and decision trees to determine clinical variables strongly related to these outcomes. A Naïve Byes classifier and decision trees were used to calculate the predicted probabilities of liver steatosis and fibrosis.</p><p><strong>Results: </strong>32% of our population had evidence of liver steatosis using 294 dB/m as a cutoff. An increase in age, serum triglyceride, and body mass index were associated with a statistically significant increase in liver steatosis; in contrast, females had statistically significantly lower values for liver steatosis by 15 points in the multivariable linear regression model. Serum LDL, smoking, and systolic and diastolic blood pressure are poorly associated with liver steatosis in the adaptive lasso regression. On the other hand, sex, tobacco use, metabolic energy expenditure, and serum triglyceride are the least associated with liver fibrosis based on decision tree analysis and a gradient-boosted model. In decision trees, people with a body mass index above 30 and HbA1c above 5.7 have a 72% likelihood of liver steatosis compared to 14% for people with a body mass index below 30. On the other hand, people with a body mass index above 41 have a 38% likelihood of liver fibrosis.</p><p><strong>Conclusion: </strong>Body mass index, hemoglobin A1c, serum triglyceride level, sex, and age could provide a good prediction for liver steatosis, while body mass index, blood pressure, platelet counts, hemoglobin A1c, serum LDL, or HDL are highly associated with liver fibrosis and should be used as an initial screening tool prior referral for VCTE/CAP.</p>","PeriodicalId":48755,"journal":{"name":"Canadian Journal of Gastroenterology and Hepatology","volume":"2023 ","pages":"1791500"},"PeriodicalIF":2.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10232144/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prediction of Liver Steatosis and Fibrosis Based on Clinical Variables Using a Large National Survey Database.\",\"authors\":\"Yanal Alnimer, Touleen Alnimer\",\"doi\":\"10.1155/2023/1791500\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Vibration-controlled transient elastography (VCTA) and controlled attenuation parameter (CAP) are used more frequently to diagnose liver fibrosis and steatosis among nonalcoholic fatty liver disease patients. However, limited robust data are available on the clinical variables strongly related to these disorders and who needs to be referred for screening.</p><p><strong>Methods: </strong>We used the National Health and Nutritional Examination Survey 2017-2018 database to identify the clinical predictors strongly related to liver steatosis and advanced fibrosis. Baseline comparisons among these groups were made based on widely accepted cutoffs. Linear and logistic regressions were performed to identify the associations between the clinical variables and liver steatosis and fibrosis. We used adaptive lasso regression, gradient-boosted model, and decision trees to determine clinical variables strongly related to these outcomes. A Naïve Byes classifier and decision trees were used to calculate the predicted probabilities of liver steatosis and fibrosis.</p><p><strong>Results: </strong>32% of our population had evidence of liver steatosis using 294 dB/m as a cutoff. An increase in age, serum triglyceride, and body mass index were associated with a statistically significant increase in liver steatosis; in contrast, females had statistically significantly lower values for liver steatosis by 15 points in the multivariable linear regression model. Serum LDL, smoking, and systolic and diastolic blood pressure are poorly associated with liver steatosis in the adaptive lasso regression. On the other hand, sex, tobacco use, metabolic energy expenditure, and serum triglyceride are the least associated with liver fibrosis based on decision tree analysis and a gradient-boosted model. In decision trees, people with a body mass index above 30 and HbA1c above 5.7 have a 72% likelihood of liver steatosis compared to 14% for people with a body mass index below 30. On the other hand, people with a body mass index above 41 have a 38% likelihood of liver fibrosis.</p><p><strong>Conclusion: </strong>Body mass index, hemoglobin A1c, serum triglyceride level, sex, and age could provide a good prediction for liver steatosis, while body mass index, blood pressure, platelet counts, hemoglobin A1c, serum LDL, or HDL are highly associated with liver fibrosis and should be used as an initial screening tool prior referral for VCTE/CAP.</p>\",\"PeriodicalId\":48755,\"journal\":{\"name\":\"Canadian Journal of Gastroenterology and Hepatology\",\"volume\":\"2023 \",\"pages\":\"1791500\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10232144/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Gastroenterology and Hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/1791500\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/1791500","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Prediction of Liver Steatosis and Fibrosis Based on Clinical Variables Using a Large National Survey Database.
Background: Vibration-controlled transient elastography (VCTA) and controlled attenuation parameter (CAP) are used more frequently to diagnose liver fibrosis and steatosis among nonalcoholic fatty liver disease patients. However, limited robust data are available on the clinical variables strongly related to these disorders and who needs to be referred for screening.
Methods: We used the National Health and Nutritional Examination Survey 2017-2018 database to identify the clinical predictors strongly related to liver steatosis and advanced fibrosis. Baseline comparisons among these groups were made based on widely accepted cutoffs. Linear and logistic regressions were performed to identify the associations between the clinical variables and liver steatosis and fibrosis. We used adaptive lasso regression, gradient-boosted model, and decision trees to determine clinical variables strongly related to these outcomes. A Naïve Byes classifier and decision trees were used to calculate the predicted probabilities of liver steatosis and fibrosis.
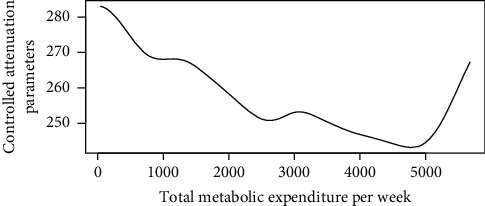
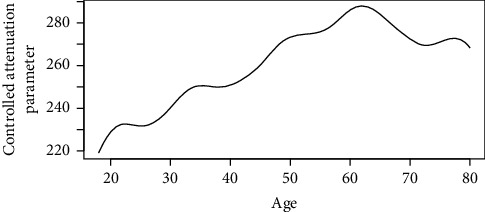
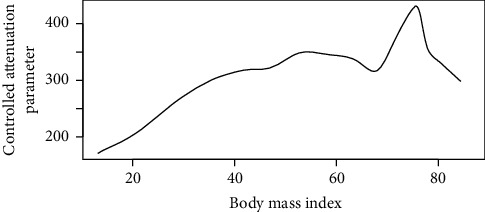
Results: 32% of our population had evidence of liver steatosis using 294 dB/m as a cutoff. An increase in age, serum triglyceride, and body mass index were associated with a statistically significant increase in liver steatosis; in contrast, females had statistically significantly lower values for liver steatosis by 15 points in the multivariable linear regression model. Serum LDL, smoking, and systolic and diastolic blood pressure are poorly associated with liver steatosis in the adaptive lasso regression. On the other hand, sex, tobacco use, metabolic energy expenditure, and serum triglyceride are the least associated with liver fibrosis based on decision tree analysis and a gradient-boosted model. In decision trees, people with a body mass index above 30 and HbA1c above 5.7 have a 72% likelihood of liver steatosis compared to 14% for people with a body mass index below 30. On the other hand, people with a body mass index above 41 have a 38% likelihood of liver fibrosis.
Conclusion: Body mass index, hemoglobin A1c, serum triglyceride level, sex, and age could provide a good prediction for liver steatosis, while body mass index, blood pressure, platelet counts, hemoglobin A1c, serum LDL, or HDL are highly associated with liver fibrosis and should be used as an initial screening tool prior referral for VCTE/CAP.
期刊介绍:
Canadian Journal of Gastroenterology and Hepatology is a peer-reviewed, open access journal that publishes original research articles, review articles, and clinical studies in all areas of gastroenterology and liver disease - medicine and surgery.
The Canadian Journal of Gastroenterology and Hepatology is sponsored by the Canadian Association of Gastroenterology and the Canadian Association for the Study of the Liver.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


