Alejandra Meza Contreras , Darrell B. Newman , Lucio Cappelloni , Alexander S. Niven , Michael R. Mueller , Ravindra Ganesh , Ray W. Squires , Amanda R. Bonikowske , Thomas G. Allison
{"title":"长程 COVID-19 与非 COVID-19 患者的心肺功能测试(未分型呼气性呼吸困难","authors":"Alejandra Meza Contreras , Darrell B. Newman , Lucio Cappelloni , Alexander S. Niven , Michael R. Mueller , Ravindra Ganesh , Ray W. Squires , Amanda R. Bonikowske , Thomas G. Allison","doi":"10.1016/j.pcad.2023.05.005","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Dyspnea and fatigue are characteristics of long SARS-CoV-2 (COVID)-19. Cardiopulmonary exercise testing (CPET) can be used to better evaluate such patients.</p></div><div><h3>Research question</h3><p>How significantly and by what mechanisms is exercise capacity impaired in patients with long COVID who are coming to a specialized clinic for evaluation?</p></div><div><h3>Study design and methods</h3><p>We performed a cohort study using the Mayo Clinic exercise testing database. Subjects included consecutive long COVID patients without prior history of heart or lung disease sent from the Post-COVID Care Clinic for CPET. They were compared to a historical group of non–COVID patients with undifferentiated dyspnea also without known cardiac or pulmonary disease. Statistical comparisons were performed by <em>t</em>-test or Pearson's chi<sup>2</sup> test controlling for age, sex, and beta blocker use where appropriate.</p></div><div><h3>Results</h3><p>We found 77 patients with long COVID and 766 control patients. Long COVID patients were younger (47 ± 15 vs 50 ± 10 years, <em>P</em> < .01) and more likely female (70% vs 58%, P < .01). The most prominent difference on CPETs was lower percent predicted peak V̇O<sub>2</sub> (73 ± 18 vs 85 ± 23%, <em>p</em> < .0001). Autonomic abnormalities (resting tachycardia, CNS changes, low systolic blood pressure) were seen during CPET more commonly in long COVID patients (34 vs 23%, <em>P</em> < .04), while mild pulmonary abnormalities (mild desaturation, limited breathing reserve, elevated V̇<sub>E</sub>/V̇CO<sub>2</sub>) during CPET were similar (19% in both groups) with only 1 long COVID patient showing severe impairment.</p></div><div><h3>Interpretation</h3><p>We identified severe exercise limitation among long COVID patients. Young women may be at higher risk for these complications. Though mild pulmonary and autonomic impairment were common in long COVID patients, marked limitations were uncommon. We hope our observations help to untangle the physiologic abnormalities responsible for the symptomatology of long COVID.</p></div>","PeriodicalId":21156,"journal":{"name":"Progress in cardiovascular diseases","volume":"83 ","pages":"Pages 71-76"},"PeriodicalIF":5.6000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10198738/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cardiopulmonary testing in long COVID-19 versus non–COVID-19 patients with undifferentiated Dyspnea on exertion\",\"authors\":\"Alejandra Meza Contreras , Darrell B. Newman , Lucio Cappelloni , Alexander S. Niven , Michael R. Mueller , Ravindra Ganesh , Ray W. Squires , Amanda R. Bonikowske , Thomas G. Allison\",\"doi\":\"10.1016/j.pcad.2023.05.005\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Dyspnea and fatigue are characteristics of long SARS-CoV-2 (COVID)-19. Cardiopulmonary exercise testing (CPET) can be used to better evaluate such patients.</p></div><div><h3>Research question</h3><p>How significantly and by what mechanisms is exercise capacity impaired in patients with long COVID who are coming to a specialized clinic for evaluation?</p></div><div><h3>Study design and methods</h3><p>We performed a cohort study using the Mayo Clinic exercise testing database. Subjects included consecutive long COVID patients without prior history of heart or lung disease sent from the Post-COVID Care Clinic for CPET. They were compared to a historical group of non–COVID patients with undifferentiated dyspnea also without known cardiac or pulmonary disease. Statistical comparisons were performed by <em>t</em>-test or Pearson's chi<sup>2</sup> test controlling for age, sex, and beta blocker use where appropriate.</p></div><div><h3>Results</h3><p>We found 77 patients with long COVID and 766 control patients. Long COVID patients were younger (47 ± 15 vs 50 ± 10 years, <em>P</em> < .01) and more likely female (70% vs 58%, P < .01). The most prominent difference on CPETs was lower percent predicted peak V̇O<sub>2</sub> (73 ± 18 vs 85 ± 23%, <em>p</em> < .0001). Autonomic abnormalities (resting tachycardia, CNS changes, low systolic blood pressure) were seen during CPET more commonly in long COVID patients (34 vs 23%, <em>P</em> < .04), while mild pulmonary abnormalities (mild desaturation, limited breathing reserve, elevated V̇<sub>E</sub>/V̇CO<sub>2</sub>) during CPET were similar (19% in both groups) with only 1 long COVID patient showing severe impairment.</p></div><div><h3>Interpretation</h3><p>We identified severe exercise limitation among long COVID patients. Young women may be at higher risk for these complications. Though mild pulmonary and autonomic impairment were common in long COVID patients, marked limitations were uncommon. We hope our observations help to untangle the physiologic abnormalities responsible for the symptomatology of long COVID.</p></div>\",\"PeriodicalId\":21156,\"journal\":{\"name\":\"Progress in cardiovascular diseases\",\"volume\":\"83 \",\"pages\":\"Pages 71-76\"},\"PeriodicalIF\":5.6000,\"publicationDate\":\"2024-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10198738/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Progress in cardiovascular diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0033062023000531\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Progress in cardiovascular diseases","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0033062023000531","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
研究背景呼吸困难和疲劳是长SARS-CoV-2(COVID)-19患者的特征。心肺运动测试(CPET)可用于更好地评估此类患者。研究问题对于来专科门诊接受评估的长病程 COVID 患者,运动能力受损的程度有多严重以及受损的机制是什么? 研究设计与方法我们利用梅奥诊所运动测试数据库进行了一项队列研究。研究对象包括由COVID后护理门诊送来进行CPET测试的无心肺疾病史的连续长COVID患者。他们与历史上一组同样没有已知心肺疾病的未分化呼吸困难的非 COVID 患者进行了比较。统计比较采用 t 检验或 Pearson's chi2 检验,并酌情控制年龄、性别和使用β受体阻滞剂的情况。长 COVID 患者更年轻(47 ± 15 岁 vs 50 ± 10 岁,P < .01),更可能是女性(70% vs 58%,P < .01)。CPET 最显著的差异是预测峰值 V̇O2 百分比较低(73 ± 18 vs 85 ± 23%,P < .0001)。CPET期间,自主神经异常(静息心动过速、中枢神经系统变化、收缩压过低)在长COVID患者中更为常见(34% vs 23%,P < .04),而CPET期间的轻度肺部异常(轻度饱和度降低、呼吸储备受限、V.̇E/V.CO2升高)与长COVID患者相似(两组均为19%),只有1名长COVID患者出现严重损伤。年轻女性可能面临更高的并发症风险。虽然轻度肺功能和自主神经功能受损在长程COVID患者中很常见,但明显的运动受限并不常见。我们希望我们的观察结果有助于解开导致长COVID症状的生理异常。
Cardiopulmonary testing in long COVID-19 versus non–COVID-19 patients with undifferentiated Dyspnea on exertion
Background
Dyspnea and fatigue are characteristics of long SARS-CoV-2 (COVID)-19. Cardiopulmonary exercise testing (CPET) can be used to better evaluate such patients.
Research question
How significantly and by what mechanisms is exercise capacity impaired in patients with long COVID who are coming to a specialized clinic for evaluation?
Study design and methods
We performed a cohort study using the Mayo Clinic exercise testing database. Subjects included consecutive long COVID patients without prior history of heart or lung disease sent from the Post-COVID Care Clinic for CPET. They were compared to a historical group of non–COVID patients with undifferentiated dyspnea also without known cardiac or pulmonary disease. Statistical comparisons were performed by t-test or Pearson's chi2 test controlling for age, sex, and beta blocker use where appropriate.
Results
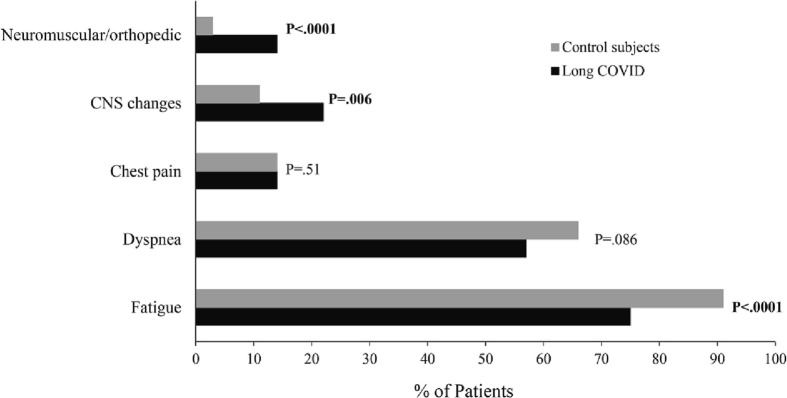
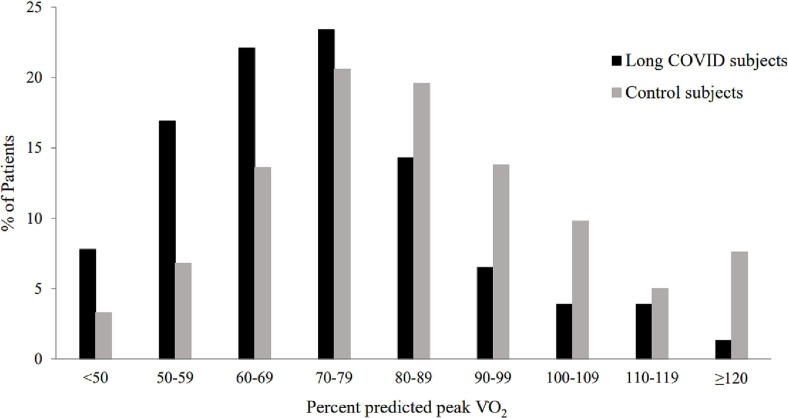
We found 77 patients with long COVID and 766 control patients. Long COVID patients were younger (47 ± 15 vs 50 ± 10 years, P < .01) and more likely female (70% vs 58%, P < .01). The most prominent difference on CPETs was lower percent predicted peak V̇O2 (73 ± 18 vs 85 ± 23%, p < .0001). Autonomic abnormalities (resting tachycardia, CNS changes, low systolic blood pressure) were seen during CPET more commonly in long COVID patients (34 vs 23%, P < .04), while mild pulmonary abnormalities (mild desaturation, limited breathing reserve, elevated V̇E/V̇CO2) during CPET were similar (19% in both groups) with only 1 long COVID patient showing severe impairment.
Interpretation
We identified severe exercise limitation among long COVID patients. Young women may be at higher risk for these complications. Though mild pulmonary and autonomic impairment were common in long COVID patients, marked limitations were uncommon. We hope our observations help to untangle the physiologic abnormalities responsible for the symptomatology of long COVID.
期刊介绍:
Progress in Cardiovascular Diseases provides comprehensive coverage of a single topic related to heart and circulatory disorders in each issue. Some issues include special articles, definitive reviews that capture the state of the art in the management of particular clinical problems in cardiology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


