Adina Mihaela Epure, Daniela Anker, Stefano Di Bernardo, Bruno R da Costa, Nicole Sekarski, Arnaud Chiolero
{"title":"降低 1 型糖尿病儿童和青少年颈动脉内膜厚度的干预措施:系统回顾与元分析》。","authors":"Adina Mihaela Epure, Daniela Anker, Stefano Di Bernardo, Bruno R da Costa, Nicole Sekarski, Arnaud Chiolero","doi":"10.3389/fcdhc.2022.882504","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hyperglycemia is associated with a higher cardiovascular risk, as evidenced by increased carotid-intima media thickness (CIMT) in youth with diabetes. We conducted a systematic review and meta-analysis to assess the effect of pharmacological or non-pharmacological interventions on CIMT in children and adolescents with prediabetes or diabetes.</p><p><strong>Methods: </strong>We conducted systematic searches of MEDLINE, EMBASE, and CENTRAL, together with supplementary searches in trial registers and other sources for studies completed up to September 2019. Interventional studies assessing ultrasound CIMT in children and adolescents with prediabetes or diabetes were considered for inclusion. Where appropriate, data were pooled across studies using random-effect meta-analysis. Quality was assessed using The Cochrane Collaboration's risk-of-bias tool and a CIMT reliability tool.</p><p><strong>Results: </strong>Six studies involving 644 children with type 1 diabetes mellitus were included. No study involved children with prediabetes or type 2 diabetes. Three randomized controlled trials (RCTs) evaluated the effects of metformin, quinapril, and atorvastatin. Three non-randomized studies, with a before-and-after design, evaluated the effects of physical exercise and continuous subcutaneous insulin infusion (CSII). The mean CIMT at baseline ranged from 0.40 to 0.51 mm. The pooled difference in CIMT was -0.01 mm (95% CI: -0.04 to 0.01) for metformin compared to placebo (2 studies; 135 participants; I<sup>2</sup>: 0%). The difference in CIMT was -0.01 mm (95% CI: -0.03 to 0.01) for quinapril compared to placebo (1 study; 406 participants). The mean change from baseline in CIMT was -0.03 mm (95% CI: -0.14 to 0.08) after physical exercise (1 study; 7 participants). Inconsistent results were reported for CSII or for atorvastatin. CIMT measurement was rated at a higher quality on all reliability domains in 3 (50%) studies. The confidence in results is limited by the low number of RCTs and their small sample sizes, as well as the high risk of bias in before-and-after studies.</p><p><strong>Conclusions: </strong>Some pharmacological interventions may decrease CIMT in children with type 1 diabetes. However, there is great uncertainty with respect to their effects and no strong conclusions can be drawn. Further evidence from larger RCTs is required.</p><p><strong>Systematic review registration: </strong>PROSPERO, CRD42017075169.</p>","PeriodicalId":73075,"journal":{"name":"Frontiers in clinical diabetes and healthcare","volume":"3 ","pages":"882504"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10012108/pdf/","citationCount":"0","resultStr":"{\"title\":\"Interventions to Decrease Carotid-Intima Media Thickness in Children and Adolescents With Type 1 Diabetes: A Systematic Review and Meta-Analysis.\",\"authors\":\"Adina Mihaela Epure, Daniela Anker, Stefano Di Bernardo, Bruno R da Costa, Nicole Sekarski, Arnaud Chiolero\",\"doi\":\"10.3389/fcdhc.2022.882504\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Hyperglycemia is associated with a higher cardiovascular risk, as evidenced by increased carotid-intima media thickness (CIMT) in youth with diabetes. We conducted a systematic review and meta-analysis to assess the effect of pharmacological or non-pharmacological interventions on CIMT in children and adolescents with prediabetes or diabetes.</p><p><strong>Methods: </strong>We conducted systematic searches of MEDLINE, EMBASE, and CENTRAL, together with supplementary searches in trial registers and other sources for studies completed up to September 2019. Interventional studies assessing ultrasound CIMT in children and adolescents with prediabetes or diabetes were considered for inclusion. Where appropriate, data were pooled across studies using random-effect meta-analysis. Quality was assessed using The Cochrane Collaboration's risk-of-bias tool and a CIMT reliability tool.</p><p><strong>Results: </strong>Six studies involving 644 children with type 1 diabetes mellitus were included. No study involved children with prediabetes or type 2 diabetes. Three randomized controlled trials (RCTs) evaluated the effects of metformin, quinapril, and atorvastatin. Three non-randomized studies, with a before-and-after design, evaluated the effects of physical exercise and continuous subcutaneous insulin infusion (CSII). The mean CIMT at baseline ranged from 0.40 to 0.51 mm. The pooled difference in CIMT was -0.01 mm (95% CI: -0.04 to 0.01) for metformin compared to placebo (2 studies; 135 participants; I<sup>2</sup>: 0%). The difference in CIMT was -0.01 mm (95% CI: -0.03 to 0.01) for quinapril compared to placebo (1 study; 406 participants). The mean change from baseline in CIMT was -0.03 mm (95% CI: -0.14 to 0.08) after physical exercise (1 study; 7 participants). Inconsistent results were reported for CSII or for atorvastatin. CIMT measurement was rated at a higher quality on all reliability domains in 3 (50%) studies. The confidence in results is limited by the low number of RCTs and their small sample sizes, as well as the high risk of bias in before-and-after studies.</p><p><strong>Conclusions: </strong>Some pharmacological interventions may decrease CIMT in children with type 1 diabetes. However, there is great uncertainty with respect to their effects and no strong conclusions can be drawn. Further evidence from larger RCTs is required.</p><p><strong>Systematic review registration: </strong>PROSPERO, CRD42017075169.</p>\",\"PeriodicalId\":73075,\"journal\":{\"name\":\"Frontiers in clinical diabetes and healthcare\",\"volume\":\"3 \",\"pages\":\"882504\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-07-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10012108/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in clinical diabetes and healthcare\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fcdhc.2022.882504\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in clinical diabetes and healthcare","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fcdhc.2022.882504","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Interventions to Decrease Carotid-Intima Media Thickness in Children and Adolescents With Type 1 Diabetes: A Systematic Review and Meta-Analysis.
Introduction: Hyperglycemia is associated with a higher cardiovascular risk, as evidenced by increased carotid-intima media thickness (CIMT) in youth with diabetes. We conducted a systematic review and meta-analysis to assess the effect of pharmacological or non-pharmacological interventions on CIMT in children and adolescents with prediabetes or diabetes.
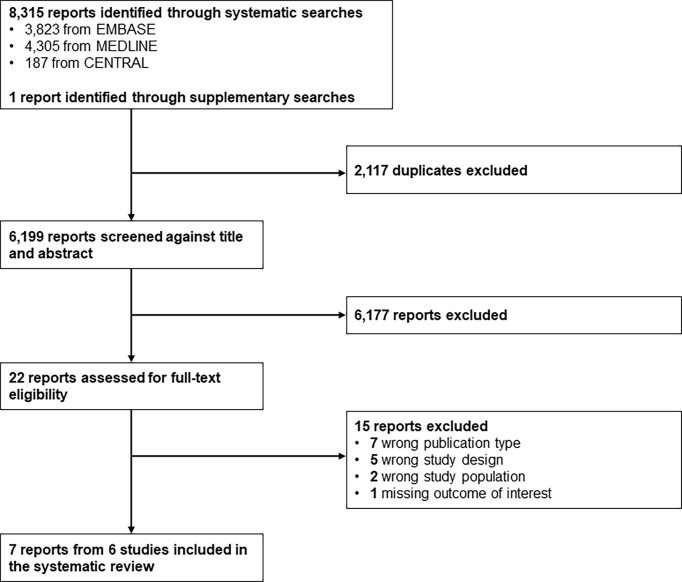
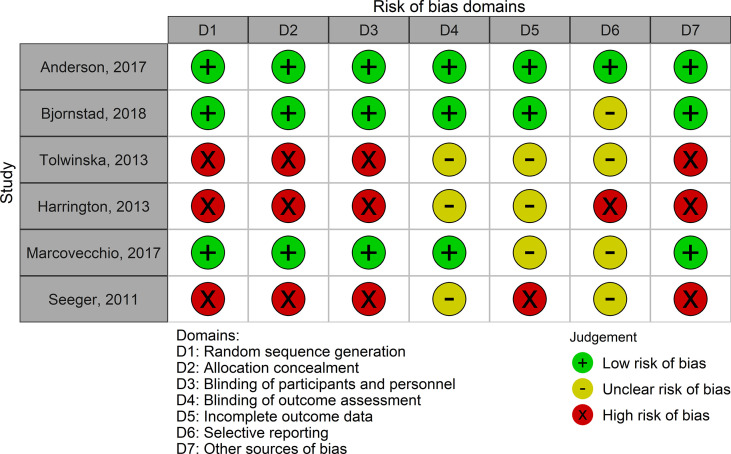
Methods: We conducted systematic searches of MEDLINE, EMBASE, and CENTRAL, together with supplementary searches in trial registers and other sources for studies completed up to September 2019. Interventional studies assessing ultrasound CIMT in children and adolescents with prediabetes or diabetes were considered for inclusion. Where appropriate, data were pooled across studies using random-effect meta-analysis. Quality was assessed using The Cochrane Collaboration's risk-of-bias tool and a CIMT reliability tool.
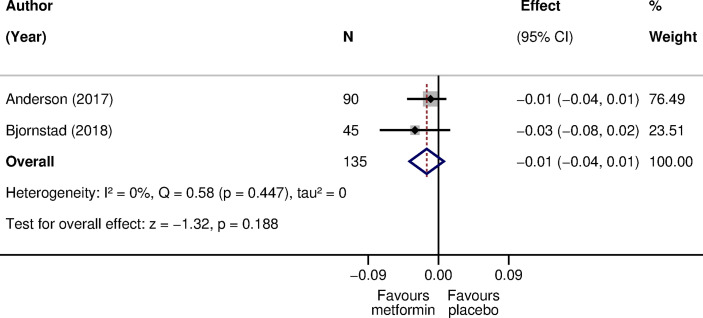
Results: Six studies involving 644 children with type 1 diabetes mellitus were included. No study involved children with prediabetes or type 2 diabetes. Three randomized controlled trials (RCTs) evaluated the effects of metformin, quinapril, and atorvastatin. Three non-randomized studies, with a before-and-after design, evaluated the effects of physical exercise and continuous subcutaneous insulin infusion (CSII). The mean CIMT at baseline ranged from 0.40 to 0.51 mm. The pooled difference in CIMT was -0.01 mm (95% CI: -0.04 to 0.01) for metformin compared to placebo (2 studies; 135 participants; I2: 0%). The difference in CIMT was -0.01 mm (95% CI: -0.03 to 0.01) for quinapril compared to placebo (1 study; 406 participants). The mean change from baseline in CIMT was -0.03 mm (95% CI: -0.14 to 0.08) after physical exercise (1 study; 7 participants). Inconsistent results were reported for CSII or for atorvastatin. CIMT measurement was rated at a higher quality on all reliability domains in 3 (50%) studies. The confidence in results is limited by the low number of RCTs and their small sample sizes, as well as the high risk of bias in before-and-after studies.
Conclusions: Some pharmacological interventions may decrease CIMT in children with type 1 diabetes. However, there is great uncertainty with respect to their effects and no strong conclusions can be drawn. Further evidence from larger RCTs is required.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


