Feike J Loots, Daan Smulders, Paul Giesen, Rogier M Hopstaken, Marleen Smits
{"title":"在非工作时间的初级保健中出现急性感染的成年患者的全身炎症反应综合征的生命体征:一项横断面研究。","authors":"Feike J Loots, Daan Smulders, Paul Giesen, Rogier M Hopstaken, Marleen Smits","doi":"10.1080/13814788.2021.1917544","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Signs of the systemic inflammatory response syndrome (SIRS) - fever (or hypothermia), tachycardia and tachypnoea - are used in the hospital setting to identify patients with possible sepsis.</p><p><strong>Objectives: </strong>To determine how frequently abnormalities in the vital signs of SIRS are present in adult out-of-hours (OOH) primary care patients with suspected infections and assess the association with acute hospital referral.</p><p><strong>Methods: </strong>We conducted a cross-sectional study at the OOH GP cooperative in Nijmegen, the Netherlands, between August and October 2015. GPs were instructed to record the body temperature, heart rate and respiratory rate of all patients with suspected acute infections. Vital signs of SIRS, other relevant signs and symptoms, and referral state were extracted from the electronic registration system of the OOH GP cooperative retrospectively. Logistic regression analysis was used to evaluate the association between clinical signs and hospital referral.</p><p><strong>Results: </strong>A total of 558 patients with suspected infections were included. At least two SIRS vital signs were abnormal in 35/409 (8.6%) of the clinic consultations and 60/149 (40.3%) of the home visits. Referral rate increased from 13% when no SIRS vital sign was abnormal to 68% when all three SIRS vital signs were abnormal. Independent associations for referral were found for decreased oxygen saturation, hypotension and rapid illness progression, but not for individual SIRS vital signs.</p><p><strong>Conclusion: </strong>Although patients with abnormal vital signs of SIRS were referred more often, decreased oxygen saturation, hypotension and rapid illness progression seem to be most important for GPs to guide further management.</p>","PeriodicalId":54380,"journal":{"name":"European Journal of General Practice","volume":"27 1","pages":"83-89"},"PeriodicalIF":2.5000,"publicationDate":"2021-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1080/13814788.2021.1917544","citationCount":"0","resultStr":"{\"title\":\"Vital signs of the systemic inflammatory response syndrome in adult patients with acute infections presenting in out-of-hours primary care: A cross-sectional study.\",\"authors\":\"Feike J Loots, Daan Smulders, Paul Giesen, Rogier M Hopstaken, Marleen Smits\",\"doi\":\"10.1080/13814788.2021.1917544\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Signs of the systemic inflammatory response syndrome (SIRS) - fever (or hypothermia), tachycardia and tachypnoea - are used in the hospital setting to identify patients with possible sepsis.</p><p><strong>Objectives: </strong>To determine how frequently abnormalities in the vital signs of SIRS are present in adult out-of-hours (OOH) primary care patients with suspected infections and assess the association with acute hospital referral.</p><p><strong>Methods: </strong>We conducted a cross-sectional study at the OOH GP cooperative in Nijmegen, the Netherlands, between August and October 2015. GPs were instructed to record the body temperature, heart rate and respiratory rate of all patients with suspected acute infections. Vital signs of SIRS, other relevant signs and symptoms, and referral state were extracted from the electronic registration system of the OOH GP cooperative retrospectively. Logistic regression analysis was used to evaluate the association between clinical signs and hospital referral.</p><p><strong>Results: </strong>A total of 558 patients with suspected infections were included. At least two SIRS vital signs were abnormal in 35/409 (8.6%) of the clinic consultations and 60/149 (40.3%) of the home visits. Referral rate increased from 13% when no SIRS vital sign was abnormal to 68% when all three SIRS vital signs were abnormal. Independent associations for referral were found for decreased oxygen saturation, hypotension and rapid illness progression, but not for individual SIRS vital signs.</p><p><strong>Conclusion: </strong>Although patients with abnormal vital signs of SIRS were referred more often, decreased oxygen saturation, hypotension and rapid illness progression seem to be most important for GPs to guide further management.</p>\",\"PeriodicalId\":54380,\"journal\":{\"name\":\"European Journal of General Practice\",\"volume\":\"27 1\",\"pages\":\"83-89\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2021-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1080/13814788.2021.1917544\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of General Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1080/13814788.2021.1917544\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of General Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/13814788.2021.1917544","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Vital signs of the systemic inflammatory response syndrome in adult patients with acute infections presenting in out-of-hours primary care: A cross-sectional study.
Background: Signs of the systemic inflammatory response syndrome (SIRS) - fever (or hypothermia), tachycardia and tachypnoea - are used in the hospital setting to identify patients with possible sepsis.
Objectives: To determine how frequently abnormalities in the vital signs of SIRS are present in adult out-of-hours (OOH) primary care patients with suspected infections and assess the association with acute hospital referral.
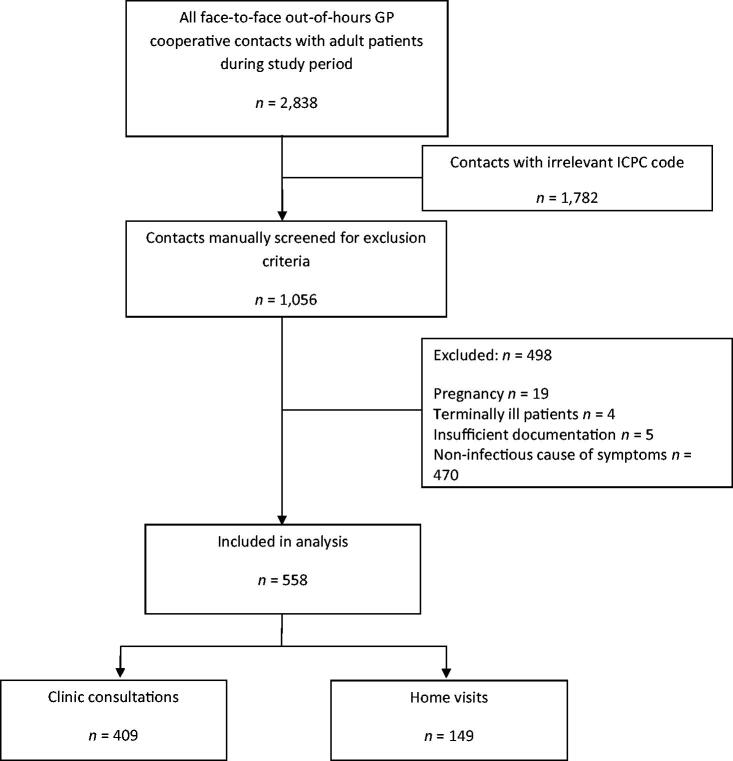
Methods: We conducted a cross-sectional study at the OOH GP cooperative in Nijmegen, the Netherlands, between August and October 2015. GPs were instructed to record the body temperature, heart rate and respiratory rate of all patients with suspected acute infections. Vital signs of SIRS, other relevant signs and symptoms, and referral state were extracted from the electronic registration system of the OOH GP cooperative retrospectively. Logistic regression analysis was used to evaluate the association between clinical signs and hospital referral.
Results: A total of 558 patients with suspected infections were included. At least two SIRS vital signs were abnormal in 35/409 (8.6%) of the clinic consultations and 60/149 (40.3%) of the home visits. Referral rate increased from 13% when no SIRS vital sign was abnormal to 68% when all three SIRS vital signs were abnormal. Independent associations for referral were found for decreased oxygen saturation, hypotension and rapid illness progression, but not for individual SIRS vital signs.
Conclusion: Although patients with abnormal vital signs of SIRS were referred more often, decreased oxygen saturation, hypotension and rapid illness progression seem to be most important for GPs to guide further management.
期刊介绍:
The EJGP aims to:
foster scientific research in primary care medicine (family medicine, general practice) in Europe
stimulate education and debate, relevant for the development of primary care medicine in Europe.
Scope
The EJGP publishes original research papers, review articles and clinical case reports on all aspects of primary care medicine (family medicine, general practice), providing new knowledge on medical decision-making, healthcare delivery, medical education, and research methodology.
Areas covered include primary care epidemiology, prevention, diagnosis, pharmacotherapy, non-drug interventions, multi- and comorbidity, palliative care, shared decision making, inter-professional collaboration, quality and safety, training and teaching, and quantitative and qualitative research methods.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


