Hossein Haghbin, Nuruddinkhodja Zakirkhodjaev, Muhammad Aziz
{"title":"结肠镜检查的退出时间,过去,现在和未来,叙述回顾。","authors":"Hossein Haghbin, Nuruddinkhodja Zakirkhodjaev, Muhammad Aziz","doi":"10.21037/tgh-23-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Colonoscopy is a time proven, safe, and gold standard screening method for colorectal cancer (CRC). In order to achieve its objectives, quality markers have been defined for colonoscopy, including withdrawal time (WT). WT is defined as the time spent from reaching the cecum or terminal ileum till the end of procedure in colonoscopies without any additional interventions. This review aims to provide evidence on WT efficacy and future directions.</p><p><strong>Methods: </strong>We conducted a comprehensive literature search of articles evaluating WT. Search was limited to English language articles from all peer-reviewed journals.</p><p><strong>Key content and findings: </strong>The seminal study by Barclay <i>et al.</i>, led to setting of a minimum WT of 6 minutes as the recommended amount for colonoscopy, per 2006 American College of Gastroenterology (ACG) taskforce. Since then, many observational studies have confirmed the efficacy of 6 minutes. Recently, multiple large multicenter trials suggest WT of 9 minutes as the alternative for better outcomes. Recently, novel Artificial Intelligence (AI) models have shown promise in improving WT and other outcomes and proved an exciting tool in the armamentarium of gastroenterologists. Some of these tools encourage the endoscopists to check the blind spots and clean the residual stool. This has shown to improve both WT and ADR. We recommend an improvement of these models to consider risk factors like adenoma detection in current and prior scopes to guide endoscopists spend time in each segment.</p><p><strong>Conclusions: </strong>In conclusion, new evidence demonstrates that WT of 9 minutes is better than 6 minutes. Future trends point toward an individualized AI-based approach combining real time and baseline data and guiding the endoscopist on how much time to spend in every segment of the colon in every colonoscopy procedure.</p>","PeriodicalId":23267,"journal":{"name":"Translational gastroenterology and hepatology","volume":"8 ","pages":"19"},"PeriodicalIF":3.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c8/4f/tgh-08-23-8.PMC10184034.pdf","citationCount":"2","resultStr":"{\"title\":\"Withdrawal time in colonoscopy, past, present, and future, a narrative review.\",\"authors\":\"Hossein Haghbin, Nuruddinkhodja Zakirkhodjaev, Muhammad Aziz\",\"doi\":\"10.21037/tgh-23-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objective: </strong>Colonoscopy is a time proven, safe, and gold standard screening method for colorectal cancer (CRC). In order to achieve its objectives, quality markers have been defined for colonoscopy, including withdrawal time (WT). WT is defined as the time spent from reaching the cecum or terminal ileum till the end of procedure in colonoscopies without any additional interventions. This review aims to provide evidence on WT efficacy and future directions.</p><p><strong>Methods: </strong>We conducted a comprehensive literature search of articles evaluating WT. Search was limited to English language articles from all peer-reviewed journals.</p><p><strong>Key content and findings: </strong>The seminal study by Barclay <i>et al.</i>, led to setting of a minimum WT of 6 minutes as the recommended amount for colonoscopy, per 2006 American College of Gastroenterology (ACG) taskforce. Since then, many observational studies have confirmed the efficacy of 6 minutes. Recently, multiple large multicenter trials suggest WT of 9 minutes as the alternative for better outcomes. Recently, novel Artificial Intelligence (AI) models have shown promise in improving WT and other outcomes and proved an exciting tool in the armamentarium of gastroenterologists. Some of these tools encourage the endoscopists to check the blind spots and clean the residual stool. This has shown to improve both WT and ADR. We recommend an improvement of these models to consider risk factors like adenoma detection in current and prior scopes to guide endoscopists spend time in each segment.</p><p><strong>Conclusions: </strong>In conclusion, new evidence demonstrates that WT of 9 minutes is better than 6 minutes. Future trends point toward an individualized AI-based approach combining real time and baseline data and guiding the endoscopist on how much time to spend in every segment of the colon in every colonoscopy procedure.</p>\",\"PeriodicalId\":23267,\"journal\":{\"name\":\"Translational gastroenterology and hepatology\",\"volume\":\"8 \",\"pages\":\"19\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c8/4f/tgh-08-23-8.PMC10184034.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational gastroenterology and hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/tgh-23-8\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tgh-23-8","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Withdrawal time in colonoscopy, past, present, and future, a narrative review.
Background and objective: Colonoscopy is a time proven, safe, and gold standard screening method for colorectal cancer (CRC). In order to achieve its objectives, quality markers have been defined for colonoscopy, including withdrawal time (WT). WT is defined as the time spent from reaching the cecum or terminal ileum till the end of procedure in colonoscopies without any additional interventions. This review aims to provide evidence on WT efficacy and future directions.
Methods: We conducted a comprehensive literature search of articles evaluating WT. Search was limited to English language articles from all peer-reviewed journals.
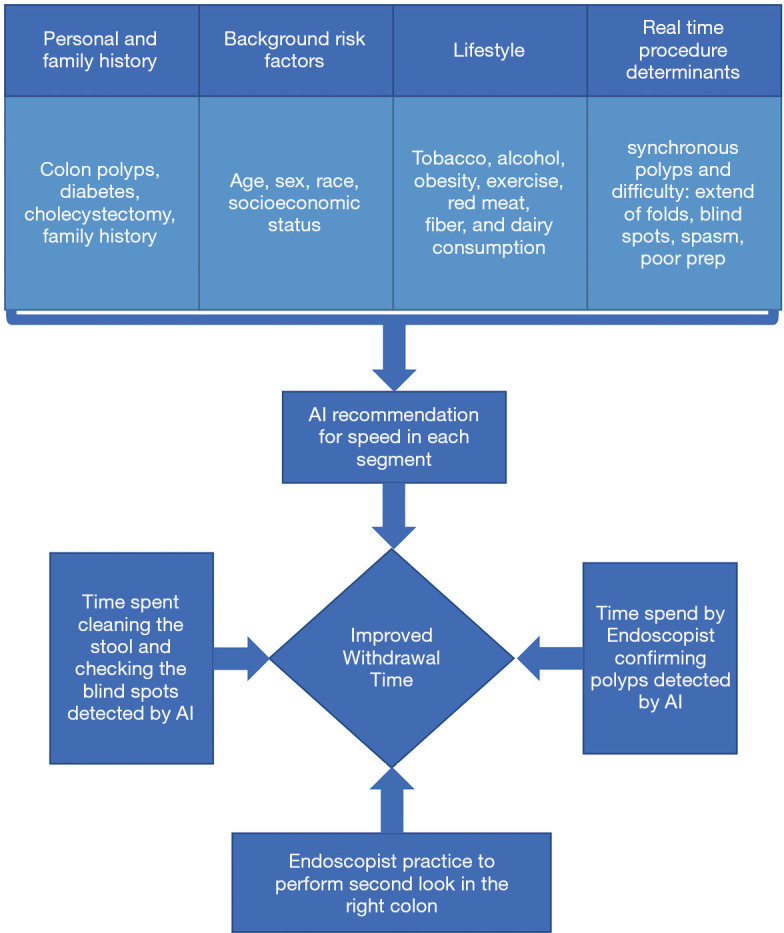
Key content and findings: The seminal study by Barclay et al., led to setting of a minimum WT of 6 minutes as the recommended amount for colonoscopy, per 2006 American College of Gastroenterology (ACG) taskforce. Since then, many observational studies have confirmed the efficacy of 6 minutes. Recently, multiple large multicenter trials suggest WT of 9 minutes as the alternative for better outcomes. Recently, novel Artificial Intelligence (AI) models have shown promise in improving WT and other outcomes and proved an exciting tool in the armamentarium of gastroenterologists. Some of these tools encourage the endoscopists to check the blind spots and clean the residual stool. This has shown to improve both WT and ADR. We recommend an improvement of these models to consider risk factors like adenoma detection in current and prior scopes to guide endoscopists spend time in each segment.
Conclusions: In conclusion, new evidence demonstrates that WT of 9 minutes is better than 6 minutes. Future trends point toward an individualized AI-based approach combining real time and baseline data and guiding the endoscopist on how much time to spend in every segment of the colon in every colonoscopy procedure.
期刊介绍:
Translational Gastroenterology and Hepatology (Transl Gastroenterol Hepatol; TGH; Online ISSN 2415-1289) is an open-access, peer-reviewed online journal that focuses on cutting-edge findings in the field of translational research in gastroenterology and hepatology and provides current and practical information on diagnosis, prevention and clinical investigations of gastrointestinal, pancreas, gallbladder and hepatic diseases. Specific areas of interest include, but not limited to, multimodality therapy, biomarkers, imaging, biology, pathology, and technical advances related to gastrointestinal and hepatic diseases. Contributions pertinent to gastroenterology and hepatology are also included from related fields such as nutrition, surgery, public health, human genetics, basic sciences, education, sociology, and nursing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


