{"title":"膀胱上裂合并尿道下裂罕见病例:典型膀胱外翻的变异。","authors":"Sudhir Singh, Jiledar Rawat, Nitin Pant","doi":"10.1136/wjps-2022-000552","DOIUrl":null,"url":null,"abstract":"© Author(s) (or their employer(s)) 2023. Reuse permitted under CC BYNC. No commercial reuse. See rights and permissions. Published by BMJ. Rare variants of bladder exstrophy are pseudoexstrophy, covered exstrophy, duplicate exstrophy, superior vesical fissure, visceral sequestration, and omphalocele, exstrophy of the cloaca, imperforate anus, and spinal defects syndrome. They comprise 10% of all cases of the exstrophy–epispadias complex. Here, we managed a 1yearold male child who presented with a 2.5 cm diameter mucosal opening in the hypogastric region, draining urine through it. The child also had distal penile hypospadias with a stenotic meatus through which he passed urine. The prepuce was hooded, and there was no chordee. On inserting a smallcaliber feeding tube through the stenotic meatus, it is visible through the hypogastric region defect. A lowlying umbilicus was present (figure 1A,B). Widening of the symphysis pubis both clinically and on an Xray was present. There was a divergence of the rectus abdominis muscle. Both testes were in the scrotum. He was continent of urine. Blood investigations were normal, including serum creatinine, and ultrasonography of the bilateral kidney and ureter was normal. The anatomy of the bladder was studied preoperatively via contrast study, although the bladder was open and not holding the contrast, so proper VCUG (voiding cystourethrogram) was not possible to perform at that time (figure 2). At 1 year of age, the child was planned for surgical correction. A circumferential bladder fissure incision with a lower abdominal midline incision was made; the upper part of the bladder was mobilized extraperitoneal. The bladder was repaired in two layers, and then the rectus muscle was approximated in the midline. Meatotomy was performed because of the stenotic meatus (figure 1C,D). The patient tolerated closure well. The child developed a right inguinal hernia at followup. The second surgery was performed at 2 years of age. Snodgrass repair for hypospadias along with right inguinal hernia was performed. The child was doing Figure 1 Clinical and operative pictures of the case of superior vesical fissure with hypospadias. (A) Lowset umbilicus and hypospadias meatus. (B) Hypospadias meatus. (C) Picture showing hypospadias meatus, meatotomy performed. (D) Intraoperative view showing repair of abdominal wall after repair of the bladder. Figure 2 Cystogram (radiograph of the bladder with contrast, not properly visualized as not holding the contrast). R, right.","PeriodicalId":23823,"journal":{"name":"World Journal of Pediatric Surgery","volume":"6 2","pages":"e000552"},"PeriodicalIF":0.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e6/0a/wjps-2022-000552.PMC10193042.pdf","citationCount":"1","resultStr":"{\"title\":\"Rare case of superior vesical fissure with hypospadias: variants of classic bladder exstrophy.\",\"authors\":\"Sudhir Singh, Jiledar Rawat, Nitin Pant\",\"doi\":\"10.1136/wjps-2022-000552\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"© Author(s) (or their employer(s)) 2023. Reuse permitted under CC BYNC. No commercial reuse. See rights and permissions. Published by BMJ. Rare variants of bladder exstrophy are pseudoexstrophy, covered exstrophy, duplicate exstrophy, superior vesical fissure, visceral sequestration, and omphalocele, exstrophy of the cloaca, imperforate anus, and spinal defects syndrome. They comprise 10% of all cases of the exstrophy–epispadias complex. Here, we managed a 1yearold male child who presented with a 2.5 cm diameter mucosal opening in the hypogastric region, draining urine through it. The child also had distal penile hypospadias with a stenotic meatus through which he passed urine. The prepuce was hooded, and there was no chordee. On inserting a smallcaliber feeding tube through the stenotic meatus, it is visible through the hypogastric region defect. A lowlying umbilicus was present (figure 1A,B). Widening of the symphysis pubis both clinically and on an Xray was present. There was a divergence of the rectus abdominis muscle. Both testes were in the scrotum. He was continent of urine. Blood investigations were normal, including serum creatinine, and ultrasonography of the bilateral kidney and ureter was normal. The anatomy of the bladder was studied preoperatively via contrast study, although the bladder was open and not holding the contrast, so proper VCUG (voiding cystourethrogram) was not possible to perform at that time (figure 2). At 1 year of age, the child was planned for surgical correction. A circumferential bladder fissure incision with a lower abdominal midline incision was made; the upper part of the bladder was mobilized extraperitoneal. The bladder was repaired in two layers, and then the rectus muscle was approximated in the midline. Meatotomy was performed because of the stenotic meatus (figure 1C,D). The patient tolerated closure well. The child developed a right inguinal hernia at followup. The second surgery was performed at 2 years of age. Snodgrass repair for hypospadias along with right inguinal hernia was performed. The child was doing Figure 1 Clinical and operative pictures of the case of superior vesical fissure with hypospadias. (A) Lowset umbilicus and hypospadias meatus. (B) Hypospadias meatus. (C) Picture showing hypospadias meatus, meatotomy performed. (D) Intraoperative view showing repair of abdominal wall after repair of the bladder. Figure 2 Cystogram (radiograph of the bladder with contrast, not properly visualized as not holding the contrast). R, right.\",\"PeriodicalId\":23823,\"journal\":{\"name\":\"World Journal of Pediatric Surgery\",\"volume\":\"6 2\",\"pages\":\"e000552\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e6/0a/wjps-2022-000552.PMC10193042.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Pediatric Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/wjps-2022-000552\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Pediatric Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/wjps-2022-000552","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 1
Rare case of superior vesical fissure with hypospadias: variants of classic bladder exstrophy.
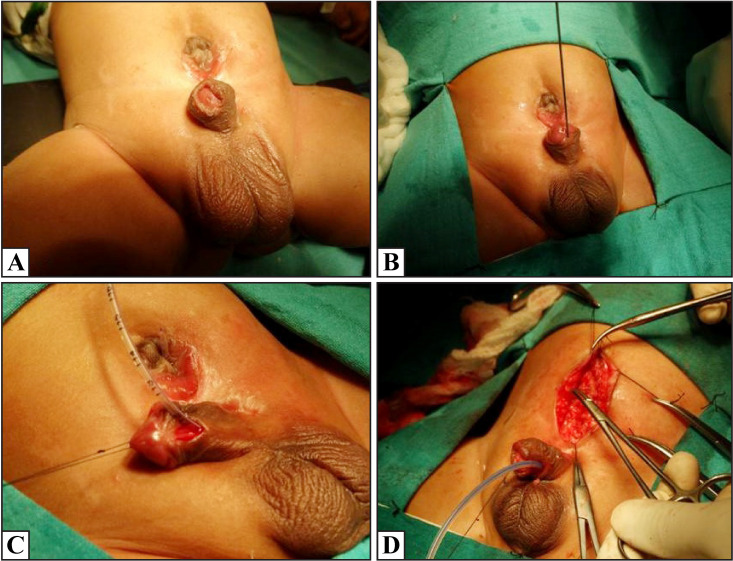
© Author(s) (or their employer(s)) 2023. Reuse permitted under CC BYNC. No commercial reuse. See rights and permissions. Published by BMJ. Rare variants of bladder exstrophy are pseudoexstrophy, covered exstrophy, duplicate exstrophy, superior vesical fissure, visceral sequestration, and omphalocele, exstrophy of the cloaca, imperforate anus, and spinal defects syndrome. They comprise 10% of all cases of the exstrophy–epispadias complex. Here, we managed a 1yearold male child who presented with a 2.5 cm diameter mucosal opening in the hypogastric region, draining urine through it. The child also had distal penile hypospadias with a stenotic meatus through which he passed urine. The prepuce was hooded, and there was no chordee. On inserting a smallcaliber feeding tube through the stenotic meatus, it is visible through the hypogastric region defect. A lowlying umbilicus was present (figure 1A,B). Widening of the symphysis pubis both clinically and on an Xray was present. There was a divergence of the rectus abdominis muscle. Both testes were in the scrotum. He was continent of urine. Blood investigations were normal, including serum creatinine, and ultrasonography of the bilateral kidney and ureter was normal. The anatomy of the bladder was studied preoperatively via contrast study, although the bladder was open and not holding the contrast, so proper VCUG (voiding cystourethrogram) was not possible to perform at that time (figure 2). At 1 year of age, the child was planned for surgical correction. A circumferential bladder fissure incision with a lower abdominal midline incision was made; the upper part of the bladder was mobilized extraperitoneal. The bladder was repaired in two layers, and then the rectus muscle was approximated in the midline. Meatotomy was performed because of the stenotic meatus (figure 1C,D). The patient tolerated closure well. The child developed a right inguinal hernia at followup. The second surgery was performed at 2 years of age. Snodgrass repair for hypospadias along with right inguinal hernia was performed. The child was doing Figure 1 Clinical and operative pictures of the case of superior vesical fissure with hypospadias. (A) Lowset umbilicus and hypospadias meatus. (B) Hypospadias meatus. (C) Picture showing hypospadias meatus, meatotomy performed. (D) Intraoperative view showing repair of abdominal wall after repair of the bladder. Figure 2 Cystogram (radiograph of the bladder with contrast, not properly visualized as not holding the contrast). R, right.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


