Richard I Farb, Sean T O'Reilly, Everardus J Hendriks, Philip W Peng, Eric M Massicotte, Yasmine Hoydonckx, Patrick J Nicholson
{"title":"csf -静脉瘘引起的自发性颅内低血压:评估卧位脊髓造影和维持卧位CT后肾脏造影剂积聚以改善瘘定位。","authors":"Richard I Farb, Sean T O'Reilly, Everardus J Hendriks, Philip W Peng, Eric M Massicotte, Yasmine Hoydonckx, Patrick J Nicholson","doi":"10.1177/15910199231172627","DOIUrl":null,"url":null,"abstract":"<p><p>PurposePresented here is a strategy of sequential lateral decubitus digital subtraction myelography (LDDSM) followed closely by lateral decubitus CT (LDCT) to facilitate cerebrospinal fluid (CSF)-venous fistula (CVF) localization.Materials and MethodsThis is a retrospective analysis of patients referred to our institution for evaluation of CSF leak. Patients with Type 1 and Type 2 leaks, and those not displaying MR brain stigmata of intracranial hypotension were excluded. All patients underwent consecutive LDDSM and LDCT. If the CVF was not localized on the first LDDSM-LDCT pair the patient returned for contralateral examinations. Images were reviewed for CVF and for accumulation of contrast within the renal pelvises expressed as a renal pelvis contrast score (RPCS) in Hounsfield units (HU).ResultsTwenty-two patients were included in this study. In 21 of 22 patients (95%) a CVF was identified yielding an RPCS for the LDDSM-LDCT pair ipsilateral to the CVF ranging from 71 to 423 with an average of 146 HU. An RPCS of the negative side LDDSM-LDCT pair contralateral to a CVF was available in 8 patients and averaged 51 HU. In 4 patients the initial bilateral LDDSM-LDCT pairs did not reveal the location of the CVF however in 3 of these 4 cases the CVF was revealed on a third LDDSM repeated ipsilateral to the higher RPCS.ConclusionThe strategy of sequential LDDSM-LDCT coupled with evaluation of renal accumulation of contrast agent appears to improve the rate of CVF localization and warrants further evaluation.</p>","PeriodicalId":14380,"journal":{"name":"Interventional Neuroradiology","volume":" ","pages":"457-463"},"PeriodicalIF":2.1000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12280252/pdf/","citationCount":"0","resultStr":"{\"title\":\"Spontaneous intracranial hypotension due to CSF-venous fistula: Evaluation of renal accumulation of contrast following decubitus myelography and maintained decubitus CT to improve fistula localization.\",\"authors\":\"Richard I Farb, Sean T O'Reilly, Everardus J Hendriks, Philip W Peng, Eric M Massicotte, Yasmine Hoydonckx, Patrick J Nicholson\",\"doi\":\"10.1177/15910199231172627\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>PurposePresented here is a strategy of sequential lateral decubitus digital subtraction myelography (LDDSM) followed closely by lateral decubitus CT (LDCT) to facilitate cerebrospinal fluid (CSF)-venous fistula (CVF) localization.Materials and MethodsThis is a retrospective analysis of patients referred to our institution for evaluation of CSF leak. Patients with Type 1 and Type 2 leaks, and those not displaying MR brain stigmata of intracranial hypotension were excluded. All patients underwent consecutive LDDSM and LDCT. If the CVF was not localized on the first LDDSM-LDCT pair the patient returned for contralateral examinations. Images were reviewed for CVF and for accumulation of contrast within the renal pelvises expressed as a renal pelvis contrast score (RPCS) in Hounsfield units (HU).ResultsTwenty-two patients were included in this study. In 21 of 22 patients (95%) a CVF was identified yielding an RPCS for the LDDSM-LDCT pair ipsilateral to the CVF ranging from 71 to 423 with an average of 146 HU. An RPCS of the negative side LDDSM-LDCT pair contralateral to a CVF was available in 8 patients and averaged 51 HU. In 4 patients the initial bilateral LDDSM-LDCT pairs did not reveal the location of the CVF however in 3 of these 4 cases the CVF was revealed on a third LDDSM repeated ipsilateral to the higher RPCS.ConclusionThe strategy of sequential LDDSM-LDCT coupled with evaluation of renal accumulation of contrast agent appears to improve the rate of CVF localization and warrants further evaluation.</p>\",\"PeriodicalId\":14380,\"journal\":{\"name\":\"Interventional Neuroradiology\",\"volume\":\" \",\"pages\":\"457-463\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12280252/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interventional Neuroradiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/15910199231172627\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/5/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interventional Neuroradiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/15910199231172627","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/21 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Spontaneous intracranial hypotension due to CSF-venous fistula: Evaluation of renal accumulation of contrast following decubitus myelography and maintained decubitus CT to improve fistula localization.
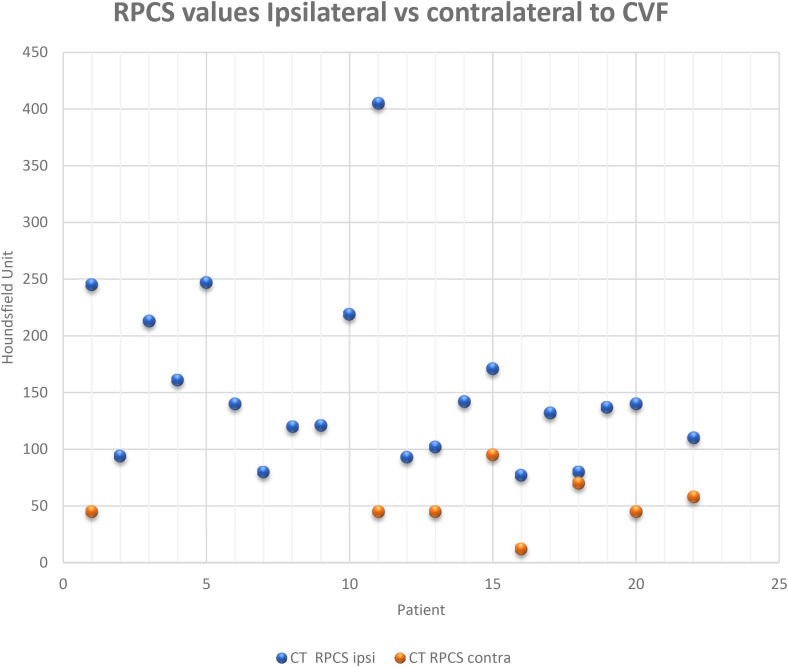
PurposePresented here is a strategy of sequential lateral decubitus digital subtraction myelography (LDDSM) followed closely by lateral decubitus CT (LDCT) to facilitate cerebrospinal fluid (CSF)-venous fistula (CVF) localization.Materials and MethodsThis is a retrospective analysis of patients referred to our institution for evaluation of CSF leak. Patients with Type 1 and Type 2 leaks, and those not displaying MR brain stigmata of intracranial hypotension were excluded. All patients underwent consecutive LDDSM and LDCT. If the CVF was not localized on the first LDDSM-LDCT pair the patient returned for contralateral examinations. Images were reviewed for CVF and for accumulation of contrast within the renal pelvises expressed as a renal pelvis contrast score (RPCS) in Hounsfield units (HU).ResultsTwenty-two patients were included in this study. In 21 of 22 patients (95%) a CVF was identified yielding an RPCS for the LDDSM-LDCT pair ipsilateral to the CVF ranging from 71 to 423 with an average of 146 HU. An RPCS of the negative side LDDSM-LDCT pair contralateral to a CVF was available in 8 patients and averaged 51 HU. In 4 patients the initial bilateral LDDSM-LDCT pairs did not reveal the location of the CVF however in 3 of these 4 cases the CVF was revealed on a third LDDSM repeated ipsilateral to the higher RPCS.ConclusionThe strategy of sequential LDDSM-LDCT coupled with evaluation of renal accumulation of contrast agent appears to improve the rate of CVF localization and warrants further evaluation.
期刊介绍:
Interventional Neuroradiology (INR) is a peer-reviewed clinical practice journal documenting the current state of interventional neuroradiology worldwide. INR publishes original clinical observations, descriptions of new techniques or procedures, case reports, and articles on the ethical and social aspects of related health care. Original research published in INR is related to the practice of interventional neuroradiology...

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


