Mehmet Serkan Özkent, Mehmet Balasar, Mehmet Giray Sönmez, Muzaffer Tansel Kilinç, Pembe Oltulu, Eren Erol, Yunus Emre Göger
{"title":"罕见的肾丢失病例:泌尿生殖器结核。","authors":"Mehmet Serkan Özkent, Mehmet Balasar, Mehmet Giray Sönmez, Muzaffer Tansel Kilinç, Pembe Oltulu, Eren Erol, Yunus Emre Göger","doi":"10.1097/j.pbj.0000000000000201","DOIUrl":null,"url":null,"abstract":"To the Editor Tuberculosis (Tbc) is a granulomatous disease caused by Mycobacterium tuberculosis bacillus (M. tuberculosis). Although it is primarily seen in the lungs, other organs may also be affected with a lower prevalence. The second most common prevalence of extrapulmonary Tbc cases, nearly 27% of extrapulmonary Tbc cases, are seen in the urogenital system. The most important mechanism introduced in urogenital Tbc pathophysiology is the hematogenous spreading after primary lung infection. After the initial settlement of bacillary in kidney parenchyma, the bacillary may not cause an infection if the host defense is satisfactory or the virulence of bacillary is low. However, the presence of these factors (low host defense or increased bacillary virulence) may cause parenchymal infiltration and granulomatous infection resulting in fibrosis. In addition, caseous necrosis in papilla and calyxes and chronic abscesses in renal parenchyma may also occur as the disease progresses. In addition to stricture in the ureteropelvic junction and ureter, it may spread to the bladder and cause bladder fibrosis and caseous necrosis. Apart from these, urogenital Tbc may be presented with epididymis and prostate involvement in male patients and the involvement of the fallopian tube, cervix, endometrium, and ovaries in female patients. Urogenital Tbc formation and development may take long periods after primary infection. The diagnosis is hard due to no specific findings. Thus, it may cause severe outcomes. The aim of this work was to present an urinary Tbc case with nonspecific symptoms for a long time and caused organ loss. Our case was a 32-year-old female patient who was admitted to the urology outpatient clinic with severe lower urinary system symptoms such as dysuria, frequency, and urgency present for 1 year. She had no additional diseases and surgery history. No pathological findings were observed in the physical examination. Because there was leukocyte positivity in urine analysis, urinary culture was taken and antibiotic treatment was started. Kidney function tests were normal in the blood biochemistry of the patient who had no bacteria growth in the urinary culture. TheHbsAg, antiHIV, and anti-HCV were negative. Since the symptoms recurred, urinary system ultrasonography was taken. Bladder irregularity, bladder wall thickening, hydronephrosis, and parenchymal thinning in the left kidney were observed in the urinary system ultrasonography.Contrasted abdominopelvic computed tomography (CT)was performed. There was left renal hydronephrosis and no ureteral dilatation in abdominopelvic CT. Asymmetrical wall thickeningwas observed in right posterior and left lateralwall in the bladder (Fig. 1). Afterward, intravenous pyelography showed no function in the left kidney (Fig. 2). In the Tc-99m DTPA, radioactivity involvement was not observed in the left kidney. It was considered that this appearance could correspond to a nonfunctional left kidney. The right kidney had normal size and morphological structure. Blood supply, concentration, and excretion functions were within normal limits in the right kidney. Right kidney GFR was calculated as 60.1 ml/min. Because therewas a left nonfunctional kidney and an irregularity in the bladder wall, a cystoscopy was planned for the patient. In cystoscopy, a nearly four cm lesion with a caseous necrotic image was observed around the left ureteral orifice. The lesion was completely resected through a 26-fr resectoscope, and specimens were sent to the pathology department. Pathological examination showed “a caseous granulomatous inflammation” (Fig. 3). Therefore, a urogenital Tbc was investigated. Tbc PCR and urinary Tbc culture were performed to investigate the Tbc. In addition, thorax CT was performed. Tbc culture and PCR results were compatible with urogenital Tbc. In thorax CT, there were multiple lymphadenopathies, a maximum size of 17 mmwith spot microcalcifications, were observed in the mediastinum and there was a soft tissue appearance at the left kidney. Afterward, the patient was consulted with the pulmonary diseases department. Isoniazid, rifampicin, ethambutol, and pyrazinamide treatment was started. After 6 months of treatment, a nephrectomy was planned for the left kidney which did not function in scintigraphy. Left open transperitoneal nephroureterectomy and lymphadenectomy were performed. The pathology result was reported as “granulomatous pyelonephritis, granulomatous inflammation, and granulomatous lymphadenitis” (Fig. 4). The patient has been followed up in correlation with urology andpulmonary diseases for the last 30months.Additional systemic treatment was not required in the postoperative period. In the Department of Urology, Konya City Hospital, Konya, Turkey, Department of Urology, Faculty of Meram Medicine, Necmettin Erbakan University, Konya, Turkey, Department of Pathology, Faculty of Meram Medicine, Necmettin Erbakan University, Konya, Turkey","PeriodicalId":74479,"journal":{"name":"Porto biomedical journal","volume":"8 1","pages":"e201"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/7c/pj9-8-e201.PMC10194725.pdf","citationCount":"0","resultStr":"{\"title\":\"A rare case of kidney loss: urogenital tuberculosis.\",\"authors\":\"Mehmet Serkan Özkent, Mehmet Balasar, Mehmet Giray Sönmez, Muzaffer Tansel Kilinç, Pembe Oltulu, Eren Erol, Yunus Emre Göger\",\"doi\":\"10.1097/j.pbj.0000000000000201\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"To the Editor Tuberculosis (Tbc) is a granulomatous disease caused by Mycobacterium tuberculosis bacillus (M. tuberculosis). Although it is primarily seen in the lungs, other organs may also be affected with a lower prevalence. The second most common prevalence of extrapulmonary Tbc cases, nearly 27% of extrapulmonary Tbc cases, are seen in the urogenital system. The most important mechanism introduced in urogenital Tbc pathophysiology is the hematogenous spreading after primary lung infection. After the initial settlement of bacillary in kidney parenchyma, the bacillary may not cause an infection if the host defense is satisfactory or the virulence of bacillary is low. However, the presence of these factors (low host defense or increased bacillary virulence) may cause parenchymal infiltration and granulomatous infection resulting in fibrosis. In addition, caseous necrosis in papilla and calyxes and chronic abscesses in renal parenchyma may also occur as the disease progresses. In addition to stricture in the ureteropelvic junction and ureter, it may spread to the bladder and cause bladder fibrosis and caseous necrosis. Apart from these, urogenital Tbc may be presented with epididymis and prostate involvement in male patients and the involvement of the fallopian tube, cervix, endometrium, and ovaries in female patients. Urogenital Tbc formation and development may take long periods after primary infection. The diagnosis is hard due to no specific findings. Thus, it may cause severe outcomes. The aim of this work was to present an urinary Tbc case with nonspecific symptoms for a long time and caused organ loss. Our case was a 32-year-old female patient who was admitted to the urology outpatient clinic with severe lower urinary system symptoms such as dysuria, frequency, and urgency present for 1 year. She had no additional diseases and surgery history. No pathological findings were observed in the physical examination. Because there was leukocyte positivity in urine analysis, urinary culture was taken and antibiotic treatment was started. Kidney function tests were normal in the blood biochemistry of the patient who had no bacteria growth in the urinary culture. TheHbsAg, antiHIV, and anti-HCV were negative. Since the symptoms recurred, urinary system ultrasonography was taken. Bladder irregularity, bladder wall thickening, hydronephrosis, and parenchymal thinning in the left kidney were observed in the urinary system ultrasonography.Contrasted abdominopelvic computed tomography (CT)was performed. There was left renal hydronephrosis and no ureteral dilatation in abdominopelvic CT. Asymmetrical wall thickeningwas observed in right posterior and left lateralwall in the bladder (Fig. 1). Afterward, intravenous pyelography showed no function in the left kidney (Fig. 2). In the Tc-99m DTPA, radioactivity involvement was not observed in the left kidney. It was considered that this appearance could correspond to a nonfunctional left kidney. The right kidney had normal size and morphological structure. Blood supply, concentration, and excretion functions were within normal limits in the right kidney. Right kidney GFR was calculated as 60.1 ml/min. Because therewas a left nonfunctional kidney and an irregularity in the bladder wall, a cystoscopy was planned for the patient. In cystoscopy, a nearly four cm lesion with a caseous necrotic image was observed around the left ureteral orifice. The lesion was completely resected through a 26-fr resectoscope, and specimens were sent to the pathology department. Pathological examination showed “a caseous granulomatous inflammation” (Fig. 3). Therefore, a urogenital Tbc was investigated. Tbc PCR and urinary Tbc culture were performed to investigate the Tbc. In addition, thorax CT was performed. Tbc culture and PCR results were compatible with urogenital Tbc. In thorax CT, there were multiple lymphadenopathies, a maximum size of 17 mmwith spot microcalcifications, were observed in the mediastinum and there was a soft tissue appearance at the left kidney. Afterward, the patient was consulted with the pulmonary diseases department. Isoniazid, rifampicin, ethambutol, and pyrazinamide treatment was started. After 6 months of treatment, a nephrectomy was planned for the left kidney which did not function in scintigraphy. Left open transperitoneal nephroureterectomy and lymphadenectomy were performed. The pathology result was reported as “granulomatous pyelonephritis, granulomatous inflammation, and granulomatous lymphadenitis” (Fig. 4). The patient has been followed up in correlation with urology andpulmonary diseases for the last 30months.Additional systemic treatment was not required in the postoperative period. In the Department of Urology, Konya City Hospital, Konya, Turkey, Department of Urology, Faculty of Meram Medicine, Necmettin Erbakan University, Konya, Turkey, Department of Pathology, Faculty of Meram Medicine, Necmettin Erbakan University, Konya, Turkey\",\"PeriodicalId\":74479,\"journal\":{\"name\":\"Porto biomedical journal\",\"volume\":\"8 1\",\"pages\":\"e201\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1a/7c/pj9-8-e201.PMC10194725.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Porto biomedical journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/j.pbj.0000000000000201\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Porto biomedical journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/j.pbj.0000000000000201","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A rare case of kidney loss: urogenital tuberculosis.
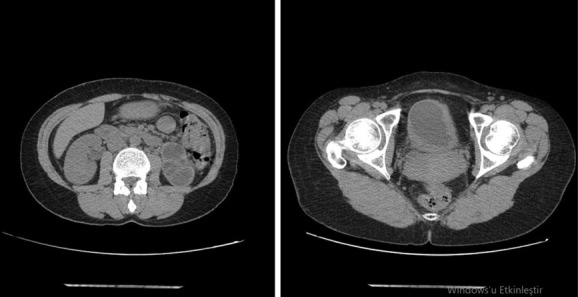
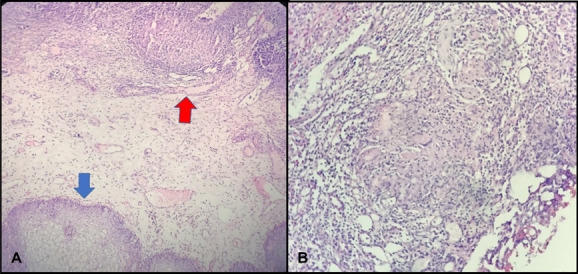
To the Editor Tuberculosis (Tbc) is a granulomatous disease caused by Mycobacterium tuberculosis bacillus (M. tuberculosis). Although it is primarily seen in the lungs, other organs may also be affected with a lower prevalence. The second most common prevalence of extrapulmonary Tbc cases, nearly 27% of extrapulmonary Tbc cases, are seen in the urogenital system. The most important mechanism introduced in urogenital Tbc pathophysiology is the hematogenous spreading after primary lung infection. After the initial settlement of bacillary in kidney parenchyma, the bacillary may not cause an infection if the host defense is satisfactory or the virulence of bacillary is low. However, the presence of these factors (low host defense or increased bacillary virulence) may cause parenchymal infiltration and granulomatous infection resulting in fibrosis. In addition, caseous necrosis in papilla and calyxes and chronic abscesses in renal parenchyma may also occur as the disease progresses. In addition to stricture in the ureteropelvic junction and ureter, it may spread to the bladder and cause bladder fibrosis and caseous necrosis. Apart from these, urogenital Tbc may be presented with epididymis and prostate involvement in male patients and the involvement of the fallopian tube, cervix, endometrium, and ovaries in female patients. Urogenital Tbc formation and development may take long periods after primary infection. The diagnosis is hard due to no specific findings. Thus, it may cause severe outcomes. The aim of this work was to present an urinary Tbc case with nonspecific symptoms for a long time and caused organ loss. Our case was a 32-year-old female patient who was admitted to the urology outpatient clinic with severe lower urinary system symptoms such as dysuria, frequency, and urgency present for 1 year. She had no additional diseases and surgery history. No pathological findings were observed in the physical examination. Because there was leukocyte positivity in urine analysis, urinary culture was taken and antibiotic treatment was started. Kidney function tests were normal in the blood biochemistry of the patient who had no bacteria growth in the urinary culture. TheHbsAg, antiHIV, and anti-HCV were negative. Since the symptoms recurred, urinary system ultrasonography was taken. Bladder irregularity, bladder wall thickening, hydronephrosis, and parenchymal thinning in the left kidney were observed in the urinary system ultrasonography.Contrasted abdominopelvic computed tomography (CT)was performed. There was left renal hydronephrosis and no ureteral dilatation in abdominopelvic CT. Asymmetrical wall thickeningwas observed in right posterior and left lateralwall in the bladder (Fig. 1). Afterward, intravenous pyelography showed no function in the left kidney (Fig. 2). In the Tc-99m DTPA, radioactivity involvement was not observed in the left kidney. It was considered that this appearance could correspond to a nonfunctional left kidney. The right kidney had normal size and morphological structure. Blood supply, concentration, and excretion functions were within normal limits in the right kidney. Right kidney GFR was calculated as 60.1 ml/min. Because therewas a left nonfunctional kidney and an irregularity in the bladder wall, a cystoscopy was planned for the patient. In cystoscopy, a nearly four cm lesion with a caseous necrotic image was observed around the left ureteral orifice. The lesion was completely resected through a 26-fr resectoscope, and specimens were sent to the pathology department. Pathological examination showed “a caseous granulomatous inflammation” (Fig. 3). Therefore, a urogenital Tbc was investigated. Tbc PCR and urinary Tbc culture were performed to investigate the Tbc. In addition, thorax CT was performed. Tbc culture and PCR results were compatible with urogenital Tbc. In thorax CT, there were multiple lymphadenopathies, a maximum size of 17 mmwith spot microcalcifications, were observed in the mediastinum and there was a soft tissue appearance at the left kidney. Afterward, the patient was consulted with the pulmonary diseases department. Isoniazid, rifampicin, ethambutol, and pyrazinamide treatment was started. After 6 months of treatment, a nephrectomy was planned for the left kidney which did not function in scintigraphy. Left open transperitoneal nephroureterectomy and lymphadenectomy were performed. The pathology result was reported as “granulomatous pyelonephritis, granulomatous inflammation, and granulomatous lymphadenitis” (Fig. 4). The patient has been followed up in correlation with urology andpulmonary diseases for the last 30months.Additional systemic treatment was not required in the postoperative period. In the Department of Urology, Konya City Hospital, Konya, Turkey, Department of Urology, Faculty of Meram Medicine, Necmettin Erbakan University, Konya, Turkey, Department of Pathology, Faculty of Meram Medicine, Necmettin Erbakan University, Konya, Turkey


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


