{"title":"肺腺癌伴囊性气隙","authors":"Xue Yang, Linlin Zhang, Fanlu Meng, Wenjing Song, Dong Li, Diansheng Zhong","doi":"10.1002/cdt3.51","DOIUrl":null,"url":null,"abstract":"<p>To the Editor,</p><p>Lung cancer associated with cystic airspaces is a group of uncommon lung malignant lesions that are easy to misdiagnose even though the use of computed tomography (CT) has been more common for lung cancer screening in the clinic. The incidence of this lesion has been reported at 0.5%–3.7% in different studies.<span><sup>1-3</sup></span> Up to 80% of patients was of pulmonary adenocarcinomas and most patients had a history of smoking.<span><sup>2</sup></span></p><p>Here, we reported a case of lung adenocarcinoma associated with cystic airspace developed at least 7 years progression from one purely thin-walled lung cavity closing to the pleura on CT images in a 53-year-old man without a smoking history. Histopathology revealed the thickened wall of the cystic airspace was lung adenocarcinoma with extensive papillary and micropapillary patterns and psammoma bodies.</p><p>A 53-year-old asymptomatic male without a smoking history has had a physical examination every 1–2 years since 2013. The patient has no history of asbestos and dust exposure. In December 2013, a local thin-wall air cavity in the right lower lobe close to the pleura (Figure 1A) and nodular thickening of the bilateral pleura with partial calcification (data not shown) were found for the first time on his CT scan. Five months later, this patient underwent a chest CT examination again and there was no obvious change compared to the CT scan in 2013 (Figure 1B). After that, he did a chest CT examination every 1–2 years. No obvious radiological change was found (Figure 1C,D). However, in Oct 2018, a nonsolid nodule was found extruding from the local wall of the cystic airspace (Figure 1E), but these changes did not attract the attention of radiologists and physicians. Two years later, this nodule increased in size, and the wall of the cystic airspace thickened, which was considered the manifestation of lung cancer (Figure 1F). From 2013 to 2020, this patient had no discomfort.</p><p>In December 2020, he was administrated to our hospital for further diagnosis and treatment. A physical examination of this case showed no obvious abnormality. Axial CT images in a lung window setting showed a thicken-walled cystic space with exophytic solid nodules along the cyst wall (Figure 1G). A soft tissue nodule was seen in the mediastinal window (Figure 1H). An irregular thick-walled cavity with local solid nodule formation after three-dimensional reconstruction can be easily detected (Figure 1I). Bilateral pleurae showed irregular thickening and multiple small nodules and calcifications (Figure 1J).</p><p>After exclusion of extrathoracic malignancies by examination of brain CT scan and single-photon emission computed tomography (SPECT) whole bone scan, resection of the cyst with nodules was performed and the malignant tumor was reported via intraoperative frozen tissue pathology. So, a right lower lobectomy with lymph node dissection was subsequently performed. Postoperative pathology confirmed that there were no metastases in the margins, broken ends of the bronchus, pleural, and peripheral lymph nodes (2–4 group [0/1], 7 group [0/8], 8 group [0/1], 11 group [0/4]). The resection specimen showed that the size of the cyst is about 2.0 × 1.5 × 1.0 cm. Histopathology examination revealed the nodule extruding from the local wall of the cystic airspace was pulmonary adenocarcinoma with extensive papillary and micropapillary patterns and psammoma bodies (Figure 2A). Hematoxylin and eosin (HE) staining of tumor specimen suggested that there was no defined lining between the tumor tissue and the cavity (Figure 2A). Immunohistochemical staining showed the tumor cells were strongly positive for thyroid transcription factor 1 (TTF-1) (Figure 2B) and NapsinA (Figure 2C), positive for cytokeratin (CK) 19, Galectin 3, Cyclin D1, carcino-embryonic antigen (CEA) and CK7 (data not shown), while negative for Tg (Figure 2D), CDX2, P40, CK5/6 and CK20 (data not shown). The ki-67 index was about 20% revealing slower cell proliferation (data not shown). The tumor cells were also negative for programmed cell death ligand 1 (PD-L1) expression with tumor cell proportion score (TPS) < 1% and combined positive score (CPS) = 10 (Figure 2E). The size of one resected grayish-yellow pleural nodule was about 0.6 cm × 0.4 cm in size and was a pure calcific nodule without metastasis of pulmonary adenocarcinoma by HE staining (Figure 2F).</p><p>A lung adenocarcinoma staged at pT1cN0M0 (Stage IA3) was diagnosed for this case. Epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) rearrangements were not found in the tumor. The tumor mutation burden (TMB) was low with 3.91 Muts/Mb. The state of microsatellite was microsatellite stable (MSS). There is no tumor recurrence until Apr 2022 (Supporting Information: Figure 1).</p><p>Lung cancers associated with cystic airspace have a higher risk of misdiagnosis due to lacking typical imaging characteristics of primary lung cancer. The diagnosis ability of F-fluorodeoxyglucose positron emission tomography/computed tomography (F-FDG PET/CT) is also limited for this type,<span><sup>4, 5</sup></span> though the maximum standardized uptake value (SUV<sub>max</sub>) is higher in patients with small-sized lung adenocarcinoma adjoining cystic airspaces.<span><sup>6</sup></span> Previous studies showed that about 22% (5/22) of missed lung carcinomas originally presented as “bulla wall thickening” on CT,<span><sup>7</sup></span> which suggested that timely detection of these lesions requires a better understanding of the early manifestation. However, little is known about the early indicators that a cystic airspace is a part of lung cancer but not a benign pulmonary cyst.<span><sup>8</sup></span> Many studies attempted to find the characteristics of lung cancer associated with cystic airspaces<span><sup>2, 9-11</sup></span>: more males than females; with a mean age of 60–70 years; over 50% of patients have a smoking history; 80% of lesions were peripheral or subpleural and distributed in all lung lobes; most patients at stage I; about 80% was adenocarcinoma followed by squamous cell carcinoma; various molecular alterations with the most common are KRAS alteration and EGFR mutations.</p><p>Four patterns of lung cancer associated with cystic airspaces were recognized by Mascalchi et al.,<span><sup>4</sup></span> according to the morphologic features of this lesion on CT scans. Type I and Type II refer to an exophytic or endophytic nodule or mass from the wall of cystic airspaces, respectively; Type III refers to cyst wall thickening without a focal nodule, which not necessarily be circumferential; and Type IV refers to solid or nonsolid nodule within a cluster of multicystic airspaces. A modified classification scheme including three aspects of airspace, consistency, and loculation was proposed by Fintelmann et al.,<span><sup>2</sup></span> based on the work of Mascalchi et al.<span><sup>4</sup></span> Mets et al.<span><sup>12</sup></span> found that Type III is most often encountered compared with the other three types and the Type III and IV lesions may be more prone to misinterpretation compared to Types I and II which is with a solid component.</p><p>However, the current classification systems, which are morphologically divided according to the entity features of images on CT, neither represent the growth speed, biological behavior, and prognosis nor cover all lesion types. Moreover, one lesion may be divided into different types due to the different layers of CT images or interobserver variability.<span><sup>12</sup></span> For this patient, the images of lung lesion presented as an eccentric thick-walled cavity and exophytic nodules (Type I) or irregular wall thickening (Type III) from different layers in CT scans of three orthogonal axes in November 2020. Furthermore, different patterns may be transformed into each other with lesions progress,<span><sup>4</sup></span> which also occurred in this case from a nonsolid nodule protruding externally from the cyst wall into a mixed type. So, three-dimensional images and thin-slice reconstructions of CT are needed for accurate classification and we should raise suspicion for cancer when the morphologic features of a cyst or pericystic nodule change. In addition, the cystic-related lesion may change after antitumor therapy. Parisi et al.<span><sup>13</sup></span> pointed out that the lesion types will change after chemotherapy and immune checkpoint inhibitor administration for advanced patients with cystic-related lung cancer, which reflects treatment response.</p><p>Studies have indicated that the cystic airspaces developed wall thickening and/or a mural nodule with a median time of 25–35 months.<span><sup>2, 4</sup></span> In fact, the evolution of a solid lung malignant lesion was consistently characterized by progressive wall thickening and/or the emergence of a nodule in or abutting the cyst wall.<span><sup>14</sup></span> In this case, the time of a definitive progression from one purely thin-walled lung cavity into lung malignant lesions was about 7 years, which reminds us a long follow-up is necessary for the isolated emphysematous bullae.</p><p>There is no prospective data on prognosis and survival for patients with lung cancer associated with cystic airspaces. Results of an earlier study of lung cancers arising in bullous emphysema indicated that the overall prognosis was not substantially different from that of patients who had lung cancer not associated with bullae.<span><sup>15</sup></span> However, a retrospective study showed that papillary (24/31) and solid (6/31) types are prevailing in patients with small-sized lung adenocarcinoma adjoining cystic airspaces and these patients have poor disease-free survival and overall survival.<span><sup>6</sup></span> In this case, the lung adenocarcinoma lesion was with extensive papillary and micropapillary patterns. There is no tumor recurrence until April 2022. Recent studies have shown that three-ITG signature (ITG subunit alpha 5 [ITGA5], ITG subunit alpha 6 [ITGA6], and ITG subunit alpha L [ITGAL]) could improve the prediction ability combined with pStage in lung adenocarcinoma and might contribute to poor prognosis by metastasis and immune escape-related pathways.<span><sup>16</sup></span></p><p>In conclusion, lung cancer associated with cystic airspaces is an uncommon manifestation of primary lung malignancy. More attention should be paid to the wall when lung cystic airspace is followed up by CT.</p><p>Xue Yang wrote the manuscript. Linlin Zhang and Fanlu Meng provided patient information and collected the data. Dong Li and Diansheng Zhong were responsible for the study conception and design. Wenjing Song reviewed the pathological sections and took pathological photos. Linlin Zhang and Diansheng Zhong critically revised the manuscript for intellectual content. All authors contributed to the article and approved the submitted version.</p><p>The authors declare no conflict of interest.</p><p>Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.</p>","PeriodicalId":32096,"journal":{"name":"Chronic Diseases and Translational Medicine","volume":"9 1","pages":"58-62"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cdt3.51","citationCount":"0","resultStr":"{\"title\":\"Lung adenocarcinoma associated with cystic airspaces\",\"authors\":\"Xue Yang, Linlin Zhang, Fanlu Meng, Wenjing Song, Dong Li, Diansheng Zhong\",\"doi\":\"10.1002/cdt3.51\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>To the Editor,</p><p>Lung cancer associated with cystic airspaces is a group of uncommon lung malignant lesions that are easy to misdiagnose even though the use of computed tomography (CT) has been more common for lung cancer screening in the clinic. The incidence of this lesion has been reported at 0.5%–3.7% in different studies.<span><sup>1-3</sup></span> Up to 80% of patients was of pulmonary adenocarcinomas and most patients had a history of smoking.<span><sup>2</sup></span></p><p>Here, we reported a case of lung adenocarcinoma associated with cystic airspace developed at least 7 years progression from one purely thin-walled lung cavity closing to the pleura on CT images in a 53-year-old man without a smoking history. Histopathology revealed the thickened wall of the cystic airspace was lung adenocarcinoma with extensive papillary and micropapillary patterns and psammoma bodies.</p><p>A 53-year-old asymptomatic male without a smoking history has had a physical examination every 1–2 years since 2013. The patient has no history of asbestos and dust exposure. In December 2013, a local thin-wall air cavity in the right lower lobe close to the pleura (Figure 1A) and nodular thickening of the bilateral pleura with partial calcification (data not shown) were found for the first time on his CT scan. Five months later, this patient underwent a chest CT examination again and there was no obvious change compared to the CT scan in 2013 (Figure 1B). After that, he did a chest CT examination every 1–2 years. No obvious radiological change was found (Figure 1C,D). However, in Oct 2018, a nonsolid nodule was found extruding from the local wall of the cystic airspace (Figure 1E), but these changes did not attract the attention of radiologists and physicians. Two years later, this nodule increased in size, and the wall of the cystic airspace thickened, which was considered the manifestation of lung cancer (Figure 1F). From 2013 to 2020, this patient had no discomfort.</p><p>In December 2020, he was administrated to our hospital for further diagnosis and treatment. A physical examination of this case showed no obvious abnormality. Axial CT images in a lung window setting showed a thicken-walled cystic space with exophytic solid nodules along the cyst wall (Figure 1G). A soft tissue nodule was seen in the mediastinal window (Figure 1H). An irregular thick-walled cavity with local solid nodule formation after three-dimensional reconstruction can be easily detected (Figure 1I). Bilateral pleurae showed irregular thickening and multiple small nodules and calcifications (Figure 1J).</p><p>After exclusion of extrathoracic malignancies by examination of brain CT scan and single-photon emission computed tomography (SPECT) whole bone scan, resection of the cyst with nodules was performed and the malignant tumor was reported via intraoperative frozen tissue pathology. So, a right lower lobectomy with lymph node dissection was subsequently performed. Postoperative pathology confirmed that there were no metastases in the margins, broken ends of the bronchus, pleural, and peripheral lymph nodes (2–4 group [0/1], 7 group [0/8], 8 group [0/1], 11 group [0/4]). The resection specimen showed that the size of the cyst is about 2.0 × 1.5 × 1.0 cm. Histopathology examination revealed the nodule extruding from the local wall of the cystic airspace was pulmonary adenocarcinoma with extensive papillary and micropapillary patterns and psammoma bodies (Figure 2A). Hematoxylin and eosin (HE) staining of tumor specimen suggested that there was no defined lining between the tumor tissue and the cavity (Figure 2A). Immunohistochemical staining showed the tumor cells were strongly positive for thyroid transcription factor 1 (TTF-1) (Figure 2B) and NapsinA (Figure 2C), positive for cytokeratin (CK) 19, Galectin 3, Cyclin D1, carcino-embryonic antigen (CEA) and CK7 (data not shown), while negative for Tg (Figure 2D), CDX2, P40, CK5/6 and CK20 (data not shown). The ki-67 index was about 20% revealing slower cell proliferation (data not shown). The tumor cells were also negative for programmed cell death ligand 1 (PD-L1) expression with tumor cell proportion score (TPS) < 1% and combined positive score (CPS) = 10 (Figure 2E). The size of one resected grayish-yellow pleural nodule was about 0.6 cm × 0.4 cm in size and was a pure calcific nodule without metastasis of pulmonary adenocarcinoma by HE staining (Figure 2F).</p><p>A lung adenocarcinoma staged at pT1cN0M0 (Stage IA3) was diagnosed for this case. Epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) rearrangements were not found in the tumor. The tumor mutation burden (TMB) was low with 3.91 Muts/Mb. The state of microsatellite was microsatellite stable (MSS). There is no tumor recurrence until Apr 2022 (Supporting Information: Figure 1).</p><p>Lung cancers associated with cystic airspace have a higher risk of misdiagnosis due to lacking typical imaging characteristics of primary lung cancer. The diagnosis ability of F-fluorodeoxyglucose positron emission tomography/computed tomography (F-FDG PET/CT) is also limited for this type,<span><sup>4, 5</sup></span> though the maximum standardized uptake value (SUV<sub>max</sub>) is higher in patients with small-sized lung adenocarcinoma adjoining cystic airspaces.<span><sup>6</sup></span> Previous studies showed that about 22% (5/22) of missed lung carcinomas originally presented as “bulla wall thickening” on CT,<span><sup>7</sup></span> which suggested that timely detection of these lesions requires a better understanding of the early manifestation. However, little is known about the early indicators that a cystic airspace is a part of lung cancer but not a benign pulmonary cyst.<span><sup>8</sup></span> Many studies attempted to find the characteristics of lung cancer associated with cystic airspaces<span><sup>2, 9-11</sup></span>: more males than females; with a mean age of 60–70 years; over 50% of patients have a smoking history; 80% of lesions were peripheral or subpleural and distributed in all lung lobes; most patients at stage I; about 80% was adenocarcinoma followed by squamous cell carcinoma; various molecular alterations with the most common are KRAS alteration and EGFR mutations.</p><p>Four patterns of lung cancer associated with cystic airspaces were recognized by Mascalchi et al.,<span><sup>4</sup></span> according to the morphologic features of this lesion on CT scans. Type I and Type II refer to an exophytic or endophytic nodule or mass from the wall of cystic airspaces, respectively; Type III refers to cyst wall thickening without a focal nodule, which not necessarily be circumferential; and Type IV refers to solid or nonsolid nodule within a cluster of multicystic airspaces. A modified classification scheme including three aspects of airspace, consistency, and loculation was proposed by Fintelmann et al.,<span><sup>2</sup></span> based on the work of Mascalchi et al.<span><sup>4</sup></span> Mets et al.<span><sup>12</sup></span> found that Type III is most often encountered compared with the other three types and the Type III and IV lesions may be more prone to misinterpretation compared to Types I and II which is with a solid component.</p><p>However, the current classification systems, which are morphologically divided according to the entity features of images on CT, neither represent the growth speed, biological behavior, and prognosis nor cover all lesion types. Moreover, one lesion may be divided into different types due to the different layers of CT images or interobserver variability.<span><sup>12</sup></span> For this patient, the images of lung lesion presented as an eccentric thick-walled cavity and exophytic nodules (Type I) or irregular wall thickening (Type III) from different layers in CT scans of three orthogonal axes in November 2020. Furthermore, different patterns may be transformed into each other with lesions progress,<span><sup>4</sup></span> which also occurred in this case from a nonsolid nodule protruding externally from the cyst wall into a mixed type. So, three-dimensional images and thin-slice reconstructions of CT are needed for accurate classification and we should raise suspicion for cancer when the morphologic features of a cyst or pericystic nodule change. In addition, the cystic-related lesion may change after antitumor therapy. Parisi et al.<span><sup>13</sup></span> pointed out that the lesion types will change after chemotherapy and immune checkpoint inhibitor administration for advanced patients with cystic-related lung cancer, which reflects treatment response.</p><p>Studies have indicated that the cystic airspaces developed wall thickening and/or a mural nodule with a median time of 25–35 months.<span><sup>2, 4</sup></span> In fact, the evolution of a solid lung malignant lesion was consistently characterized by progressive wall thickening and/or the emergence of a nodule in or abutting the cyst wall.<span><sup>14</sup></span> In this case, the time of a definitive progression from one purely thin-walled lung cavity into lung malignant lesions was about 7 years, which reminds us a long follow-up is necessary for the isolated emphysematous bullae.</p><p>There is no prospective data on prognosis and survival for patients with lung cancer associated with cystic airspaces. Results of an earlier study of lung cancers arising in bullous emphysema indicated that the overall prognosis was not substantially different from that of patients who had lung cancer not associated with bullae.<span><sup>15</sup></span> However, a retrospective study showed that papillary (24/31) and solid (6/31) types are prevailing in patients with small-sized lung adenocarcinoma adjoining cystic airspaces and these patients have poor disease-free survival and overall survival.<span><sup>6</sup></span> In this case, the lung adenocarcinoma lesion was with extensive papillary and micropapillary patterns. There is no tumor recurrence until April 2022. Recent studies have shown that three-ITG signature (ITG subunit alpha 5 [ITGA5], ITG subunit alpha 6 [ITGA6], and ITG subunit alpha L [ITGAL]) could improve the prediction ability combined with pStage in lung adenocarcinoma and might contribute to poor prognosis by metastasis and immune escape-related pathways.<span><sup>16</sup></span></p><p>In conclusion, lung cancer associated with cystic airspaces is an uncommon manifestation of primary lung malignancy. More attention should be paid to the wall when lung cystic airspace is followed up by CT.</p><p>Xue Yang wrote the manuscript. Linlin Zhang and Fanlu Meng provided patient information and collected the data. Dong Li and Diansheng Zhong were responsible for the study conception and design. Wenjing Song reviewed the pathological sections and took pathological photos. Linlin Zhang and Diansheng Zhong critically revised the manuscript for intellectual content. All authors contributed to the article and approved the submitted version.</p><p>The authors declare no conflict of interest.</p><p>Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.</p>\",\"PeriodicalId\":32096,\"journal\":{\"name\":\"Chronic Diseases and Translational Medicine\",\"volume\":\"9 1\",\"pages\":\"58-62\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-11-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cdt3.51\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chronic Diseases and Translational Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.51\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Diseases and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.51","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
致编辑:肺癌伴囊性气隙是一组不常见的肺部恶性病变,即使使用计算机断层扫描(CT)在临床肺癌筛查中更为常见,但仍容易误诊。在不同的研究中,这种病变的发生率报道为0.5%-3.7%。高达80%的患者为肺腺癌,大多数患者有吸烟史。2在此,我们报告了一例肺腺癌伴囊性空腔的病例,在CT图像上从一个靠近胸膜的纯薄壁肺腔发展到至少7年的进展,患者53岁,无吸烟史。组织病理学显示囊腔壁增厚为肺腺癌,伴广泛乳头状和微乳头状形态及沙粒小体。男,53岁,无吸烟史,自2013年起每1-2年体检一次。患者无石棉及粉尘接触史。2013年12月,CT扫描首次发现右下肺叶靠近胸膜处局部出现薄壁空腔(图1A),双侧胸膜结节性增厚伴部分钙化(数据未显示)。5个月后,该患者再次行胸部CT检查,与2013年CT扫描相比无明显变化(图1B)。此后,他每1-2年做一次胸部CT检查。未见明显影像学改变(图1C、D)。然而,在2018年10月,发现一个非实性结节从囊腔局部壁突出(图1E),但这些变化并未引起放射科医生和医生的注意。2年后,结节增大,囊腔壁增厚,考虑肺癌的表现(图1F)。从2013年到2020年,该患者没有任何不适。2020年12月到我院进一步诊治。本例体格检查未见明显异常。肺窗位轴位CT图像显示囊壁增厚,囊壁有外生性实性结节(图1G)。纵隔窗见软组织结节(图1H)。三维重建后,可见不规则厚壁腔,局部形成实性结节(图1I)。双侧胸膜不规则增厚,多发小结节及钙化(图1J)。经颅脑CT和单光子发射计算机断层扫描(SPECT)全骨扫描排除胸外恶性肿瘤后,行囊肿伴结节切除术,术中冷冻组织病理报告恶性肿瘤。因此,随后进行了右下肺叶切除术和淋巴结清扫术。术后病理证实边缘、支气管断端、胸膜及周围淋巴结无转移(2-4组[0/1]、7组[0/8]、8组[0/1]、11组[0/4])。切除标本显示囊肿大小约为2.0 × 1.5 × 1.0 cm。组织病理学检查显示,从囊腔局部壁突出的结节为肺腺癌,伴广泛的乳头状和微乳头状形态及沙粒体(图2A)。肿瘤标本苏木精和伊红(HE)染色提示肿瘤组织与腔间无明显衬层(图2A)。免疫组化染色显示,肿瘤细胞甲状腺转录因子1 (TTF-1)(图2B)和NapsinA(图2C)呈强阳性,细胞角蛋白(CK) 19、半乳糖凝集素3、细胞周期蛋白D1、癌胚抗原(CEA)和CK7呈阳性(数据未显示),而Tg(图2D)、CDX2、P40、CK5/6和CK20呈阴性(数据未显示)。ki-67指数约为20%,表明细胞增殖较慢(数据未显示)。肿瘤细胞程序性细胞死亡配体1 (PD-L1)表达阴性,肿瘤细胞比例评分(TPS) < 1%,综合阳性评分(CPS) = 10(图2E)。1例切除的灰黄色胸膜结节大小约0.6 cm × 0.4 cm, HE染色为纯钙化结节,未见肺腺癌转移(图2F)。诊断为pT1cN0M0期肺腺癌(IA3期)。肿瘤中未发现表皮生长因子受体(EGFR)突变和间变性淋巴瘤激酶(ALK)重排。肿瘤突变负荷(TMB)较低,为3.91 Muts/Mb。微卫星处于微卫星稳定状态(MSS)。截至2022年4月,该病例无复发(支持信息:图1)。由于缺乏原发性肺癌的典型影像学特征,囊性空腔相关肺癌的误诊风险较高。 f -氟脱氧葡萄糖正电子发射断层扫描/计算机断层扫描(F-FDG PET/CT)对这种类型的诊断能力也有限,尽管在毗邻囊性气隙的小肺腺癌患者中最大标准化摄取值(SUVmax)更高既往研究显示,约22%(5/22)的漏诊肺癌在CT上最初表现为“大球壁增厚”,7提示及时发现这些病变需要更好地了解其早期表现。然而,关于囊性空腔是肺癌的一部分而不是良性肺囊肿的早期指标,我们所知甚少许多研究试图发现与囊性气隙相关的肺癌的特征:男性多于女性;平均年龄60-70岁;超过50%的患者有吸烟史;80%的病变位于周围或胸膜下,分布于所有肺叶;大多数患者处于I期;约80%为腺癌,其次为鳞状细胞癌;最常见的是KRAS改变和EGFR突变。Mascalchi等人4根据肺囊性空腔病变的CT扫描形态学特征,识别出四种肺癌伴囊性空腔。I型和II型分别是指囊腔壁上的外生或内生结节或肿块;III型为囊壁增厚,无局灶性结节,不一定是周向的;IV型是指多囊性空气空间簇内的固体或非固体结节。Fintelmann等人在Mascalchi等人4 Mets等人12的基础上提出了包括空域、一致性和定位三个方面的改进分类方案2,发现与其他三种类型相比,III型病变最常见,与具有固体成分的I型和II型病变相比,III型和IV型病变可能更容易被误解。然而,目前的分类体系是根据CT图像的实体特征进行形态学划分的,既不能代表肿瘤的生长速度、生物学行为和预后,也不能涵盖所有病变类型。此外,由于CT图像的不同层数或观察者之间的差异,同一病变可能被划分为不同的类型该患者于2020年11月在三正交轴CT扫描中,肺病变表现为偏心厚壁腔及外生结节(I型)或不规则壁增厚(III型),来自不同层。此外,随着病变的进展,不同类型的结节也可能相互转化,4本病例也发生了从囊肿壁外突出的非实性结节向混合型的转变。因此,需要三维图像和CT薄层重建来进行准确的分类,当囊肿或囊周结节的形态学改变时,我们应怀疑是否为癌症。此外,囊性病变在抗肿瘤治疗后可能发生改变。Parisi et al.13指出晚期囊性肺癌患者在化疗和免疫检查点抑制剂治疗后病变类型会发生变化,这反映了治疗反应。研究表明,囊性气隙发生壁增厚和/或壁结节,中位时间为25-35个月。事实上,肺实性恶性病变的发展始终表现为肺壁逐渐增厚和/或囊肿壁内或邻近囊肿壁出现结节本病例从单纯的薄壁肺腔发展为肺恶性病变的时间约为7年,提示孤立性肺气肿大泡的随访时间较长。目前尚无关于囊性空腔相关肺癌患者预后和生存的前瞻性数据。早期对大疱性肺气肿引起的肺癌的研究结果表明,大疱性肺气肿患者的总体预后与非大疱性肺气肿患者的预后没有实质性差异然而,一项回顾性研究显示,乳头状(24/31)和实性(6/31)型在毗邻囊性气隙的小肺腺癌患者中普遍存在,这些患者的无病生存率和总生存率较差本例肺腺癌病变呈广泛的乳头状和微乳头状。到2022年4月为止没有肿瘤复发。近期研究表明,ITG的三个特征(ITG亚基α 5 [ITGA5]、ITG亚基α 6 [ITGA6]、ITG亚基α L [ITGAL])联合pStage可提高对肺腺癌的预测能力,并可能通过转移和免疫逃逸相关途径导致预后不良。 总之,肺癌伴囊性气隙是一种罕见的原发性肺恶性肿瘤的表现。CT随诊肺囊性空腔时应注意壁。手稿是薛阳写的。Linlin Zhang和Fanlu孟提供患者信息并收集数据。李东和钟殿生负责研究的构思和设计。宋文静复查病理切片并拍摄病理照片。张琳琳和钟殿生对手稿的知识内容进行了批判性的修改。所有作者都对文章做出了贡献,并批准了提交的版本。作者声明无利益冲突。对于本文中包含的任何可能可识别的图像或数据的发布,已获得个人的书面知情同意。
Lung adenocarcinoma associated with cystic airspaces
To the Editor,
Lung cancer associated with cystic airspaces is a group of uncommon lung malignant lesions that are easy to misdiagnose even though the use of computed tomography (CT) has been more common for lung cancer screening in the clinic. The incidence of this lesion has been reported at 0.5%–3.7% in different studies.1-3 Up to 80% of patients was of pulmonary adenocarcinomas and most patients had a history of smoking.2
Here, we reported a case of lung adenocarcinoma associated with cystic airspace developed at least 7 years progression from one purely thin-walled lung cavity closing to the pleura on CT images in a 53-year-old man without a smoking history. Histopathology revealed the thickened wall of the cystic airspace was lung adenocarcinoma with extensive papillary and micropapillary patterns and psammoma bodies.
A 53-year-old asymptomatic male without a smoking history has had a physical examination every 1–2 years since 2013. The patient has no history of asbestos and dust exposure. In December 2013, a local thin-wall air cavity in the right lower lobe close to the pleura (Figure 1A) and nodular thickening of the bilateral pleura with partial calcification (data not shown) were found for the first time on his CT scan. Five months later, this patient underwent a chest CT examination again and there was no obvious change compared to the CT scan in 2013 (Figure 1B). After that, he did a chest CT examination every 1–2 years. No obvious radiological change was found (Figure 1C,D). However, in Oct 2018, a nonsolid nodule was found extruding from the local wall of the cystic airspace (Figure 1E), but these changes did not attract the attention of radiologists and physicians. Two years later, this nodule increased in size, and the wall of the cystic airspace thickened, which was considered the manifestation of lung cancer (Figure 1F). From 2013 to 2020, this patient had no discomfort.
In December 2020, he was administrated to our hospital for further diagnosis and treatment. A physical examination of this case showed no obvious abnormality. Axial CT images in a lung window setting showed a thicken-walled cystic space with exophytic solid nodules along the cyst wall (Figure 1G). A soft tissue nodule was seen in the mediastinal window (Figure 1H). An irregular thick-walled cavity with local solid nodule formation after three-dimensional reconstruction can be easily detected (Figure 1I). Bilateral pleurae showed irregular thickening and multiple small nodules and calcifications (Figure 1J).
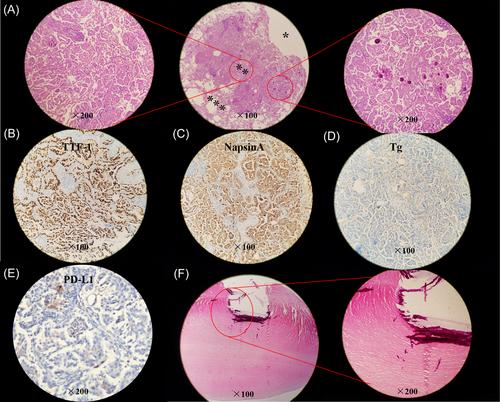
After exclusion of extrathoracic malignancies by examination of brain CT scan and single-photon emission computed tomography (SPECT) whole bone scan, resection of the cyst with nodules was performed and the malignant tumor was reported via intraoperative frozen tissue pathology. So, a right lower lobectomy with lymph node dissection was subsequently performed. Postoperative pathology confirmed that there were no metastases in the margins, broken ends of the bronchus, pleural, and peripheral lymph nodes (2–4 group [0/1], 7 group [0/8], 8 group [0/1], 11 group [0/4]). The resection specimen showed that the size of the cyst is about 2.0 × 1.5 × 1.0 cm. Histopathology examination revealed the nodule extruding from the local wall of the cystic airspace was pulmonary adenocarcinoma with extensive papillary and micropapillary patterns and psammoma bodies (Figure 2A). Hematoxylin and eosin (HE) staining of tumor specimen suggested that there was no defined lining between the tumor tissue and the cavity (Figure 2A). Immunohistochemical staining showed the tumor cells were strongly positive for thyroid transcription factor 1 (TTF-1) (Figure 2B) and NapsinA (Figure 2C), positive for cytokeratin (CK) 19, Galectin 3, Cyclin D1, carcino-embryonic antigen (CEA) and CK7 (data not shown), while negative for Tg (Figure 2D), CDX2, P40, CK5/6 and CK20 (data not shown). The ki-67 index was about 20% revealing slower cell proliferation (data not shown). The tumor cells were also negative for programmed cell death ligand 1 (PD-L1) expression with tumor cell proportion score (TPS) < 1% and combined positive score (CPS) = 10 (Figure 2E). The size of one resected grayish-yellow pleural nodule was about 0.6 cm × 0.4 cm in size and was a pure calcific nodule without metastasis of pulmonary adenocarcinoma by HE staining (Figure 2F).
A lung adenocarcinoma staged at pT1cN0M0 (Stage IA3) was diagnosed for this case. Epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) rearrangements were not found in the tumor. The tumor mutation burden (TMB) was low with 3.91 Muts/Mb. The state of microsatellite was microsatellite stable (MSS). There is no tumor recurrence until Apr 2022 (Supporting Information: Figure 1).
Lung cancers associated with cystic airspace have a higher risk of misdiagnosis due to lacking typical imaging characteristics of primary lung cancer. The diagnosis ability of F-fluorodeoxyglucose positron emission tomography/computed tomography (F-FDG PET/CT) is also limited for this type,4, 5 though the maximum standardized uptake value (SUVmax) is higher in patients with small-sized lung adenocarcinoma adjoining cystic airspaces.6 Previous studies showed that about 22% (5/22) of missed lung carcinomas originally presented as “bulla wall thickening” on CT,7 which suggested that timely detection of these lesions requires a better understanding of the early manifestation. However, little is known about the early indicators that a cystic airspace is a part of lung cancer but not a benign pulmonary cyst.8 Many studies attempted to find the characteristics of lung cancer associated with cystic airspaces2, 9-11: more males than females; with a mean age of 60–70 years; over 50% of patients have a smoking history; 80% of lesions were peripheral or subpleural and distributed in all lung lobes; most patients at stage I; about 80% was adenocarcinoma followed by squamous cell carcinoma; various molecular alterations with the most common are KRAS alteration and EGFR mutations.
Four patterns of lung cancer associated with cystic airspaces were recognized by Mascalchi et al.,4 according to the morphologic features of this lesion on CT scans. Type I and Type II refer to an exophytic or endophytic nodule or mass from the wall of cystic airspaces, respectively; Type III refers to cyst wall thickening without a focal nodule, which not necessarily be circumferential; and Type IV refers to solid or nonsolid nodule within a cluster of multicystic airspaces. A modified classification scheme including three aspects of airspace, consistency, and loculation was proposed by Fintelmann et al.,2 based on the work of Mascalchi et al.4 Mets et al.12 found that Type III is most often encountered compared with the other three types and the Type III and IV lesions may be more prone to misinterpretation compared to Types I and II which is with a solid component.
However, the current classification systems, which are morphologically divided according to the entity features of images on CT, neither represent the growth speed, biological behavior, and prognosis nor cover all lesion types. Moreover, one lesion may be divided into different types due to the different layers of CT images or interobserver variability.12 For this patient, the images of lung lesion presented as an eccentric thick-walled cavity and exophytic nodules (Type I) or irregular wall thickening (Type III) from different layers in CT scans of three orthogonal axes in November 2020. Furthermore, different patterns may be transformed into each other with lesions progress,4 which also occurred in this case from a nonsolid nodule protruding externally from the cyst wall into a mixed type. So, three-dimensional images and thin-slice reconstructions of CT are needed for accurate classification and we should raise suspicion for cancer when the morphologic features of a cyst or pericystic nodule change. In addition, the cystic-related lesion may change after antitumor therapy. Parisi et al.13 pointed out that the lesion types will change after chemotherapy and immune checkpoint inhibitor administration for advanced patients with cystic-related lung cancer, which reflects treatment response.
Studies have indicated that the cystic airspaces developed wall thickening and/or a mural nodule with a median time of 25–35 months.2, 4 In fact, the evolution of a solid lung malignant lesion was consistently characterized by progressive wall thickening and/or the emergence of a nodule in or abutting the cyst wall.14 In this case, the time of a definitive progression from one purely thin-walled lung cavity into lung malignant lesions was about 7 years, which reminds us a long follow-up is necessary for the isolated emphysematous bullae.
There is no prospective data on prognosis and survival for patients with lung cancer associated with cystic airspaces. Results of an earlier study of lung cancers arising in bullous emphysema indicated that the overall prognosis was not substantially different from that of patients who had lung cancer not associated with bullae.15 However, a retrospective study showed that papillary (24/31) and solid (6/31) types are prevailing in patients with small-sized lung adenocarcinoma adjoining cystic airspaces and these patients have poor disease-free survival and overall survival.6 In this case, the lung adenocarcinoma lesion was with extensive papillary and micropapillary patterns. There is no tumor recurrence until April 2022. Recent studies have shown that three-ITG signature (ITG subunit alpha 5 [ITGA5], ITG subunit alpha 6 [ITGA6], and ITG subunit alpha L [ITGAL]) could improve the prediction ability combined with pStage in lung adenocarcinoma and might contribute to poor prognosis by metastasis and immune escape-related pathways.16
In conclusion, lung cancer associated with cystic airspaces is an uncommon manifestation of primary lung malignancy. More attention should be paid to the wall when lung cystic airspace is followed up by CT.
Xue Yang wrote the manuscript. Linlin Zhang and Fanlu Meng provided patient information and collected the data. Dong Li and Diansheng Zhong were responsible for the study conception and design. Wenjing Song reviewed the pathological sections and took pathological photos. Linlin Zhang and Diansheng Zhong critically revised the manuscript for intellectual content. All authors contributed to the article and approved the submitted version.
The authors declare no conflict of interest.
Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
期刊介绍:
This journal aims to promote progress from basic research to clinical practice and to provide a forum for communication among basic, translational, and clinical research practitioners and physicians from all relevant disciplines. Chronic diseases such as cardiovascular diseases, cancer, diabetes, stroke, chronic respiratory diseases (such as asthma and COPD), chronic kidney diseases, and related translational research. Topics of interest for Chronic Diseases and Translational Medicine include Research and commentary on models of chronic diseases with significant implications for disease diagnosis and treatment Investigative studies of human biology with an emphasis on disease Perspectives and reviews on research topics that discuss the implications of findings from the viewpoints of basic science and clinical practic.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


