{"title":"强的松龙单独治疗伴有T滤泡辅助表型的淋巴结周围T细胞淋巴瘤的益处。","authors":"Wataru Kitamura, Hiroki Kobayashi, Tomohiro Urata, Yumiko Sato, Yusuke Naoi, Tadashi Yoshino, Yoshinobu Maeda, Shoichi Kuyama","doi":"10.3960/jslrt.22038","DOIUrl":null,"url":null,"abstract":"<p><p>A 71-year-old Japanese man presented with severe thrombocytopenia. A whole-body CT at presentation showed small cervical, axillary, and para-aortic lymphadenopathy, leading to suspicion of immune thrombocytopenia due to lymphoma. Biopsy was difficult to perform because of severe thrombocytopenia. Thus, he received prednisolone (PSL) therapy and his platelet count gradually recovered. Two and a half years after PSL therapy initiation, his cervical lymphadenopathy slightly progressed without other clinical symptoms. Hence, a biopsy from the left cervical lymph node was performed, and he was diagnosed with nodal peripheral T-cell lymphoma (PTCL) with T follicular helper (TFH) phenotype. Due to various complications, we continued treatment with prednisolone alone after the diagnosis of lymphoma; however, there was no further increase in lymph node enlargement and no other lymphoma-related symptoms for one and a half years after diagnosis. Although immunosuppressive therapy has been reported to produce a response in some patients with angioimmunoblastic T-cell lymphoma, our experience suggests that a similar subset may exist in patients with nodal PTCL with TFH phenotype, which has the same cellular origin. Immunosuppressive therapies may constitute an alternative treatment option even in the era of novel molecular-targeted therapies, especially for elderly patients who are ineligible for chemotherapy.</p>","PeriodicalId":45936,"journal":{"name":"Journal of Clinical and Experimental Hematopathology","volume":"63 1","pages":"37-42"},"PeriodicalIF":0.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/21/ac/jslrt-63-37.PMC10158724.pdf","citationCount":"0","resultStr":"{\"title\":\"Benefit of prednisolone alone in nodal peripheral T-cell lymphoma with T follicular helper phenotype.\",\"authors\":\"Wataru Kitamura, Hiroki Kobayashi, Tomohiro Urata, Yumiko Sato, Yusuke Naoi, Tadashi Yoshino, Yoshinobu Maeda, Shoichi Kuyama\",\"doi\":\"10.3960/jslrt.22038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 71-year-old Japanese man presented with severe thrombocytopenia. A whole-body CT at presentation showed small cervical, axillary, and para-aortic lymphadenopathy, leading to suspicion of immune thrombocytopenia due to lymphoma. Biopsy was difficult to perform because of severe thrombocytopenia. Thus, he received prednisolone (PSL) therapy and his platelet count gradually recovered. Two and a half years after PSL therapy initiation, his cervical lymphadenopathy slightly progressed without other clinical symptoms. Hence, a biopsy from the left cervical lymph node was performed, and he was diagnosed with nodal peripheral T-cell lymphoma (PTCL) with T follicular helper (TFH) phenotype. Due to various complications, we continued treatment with prednisolone alone after the diagnosis of lymphoma; however, there was no further increase in lymph node enlargement and no other lymphoma-related symptoms for one and a half years after diagnosis. Although immunosuppressive therapy has been reported to produce a response in some patients with angioimmunoblastic T-cell lymphoma, our experience suggests that a similar subset may exist in patients with nodal PTCL with TFH phenotype, which has the same cellular origin. Immunosuppressive therapies may constitute an alternative treatment option even in the era of novel molecular-targeted therapies, especially for elderly patients who are ineligible for chemotherapy.</p>\",\"PeriodicalId\":45936,\"journal\":{\"name\":\"Journal of Clinical and Experimental Hematopathology\",\"volume\":\"63 1\",\"pages\":\"37-42\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/21/ac/jslrt-63-37.PMC10158724.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical and Experimental Hematopathology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3960/jslrt.22038\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Experimental Hematopathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3960/jslrt.22038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Benefit of prednisolone alone in nodal peripheral T-cell lymphoma with T follicular helper phenotype.
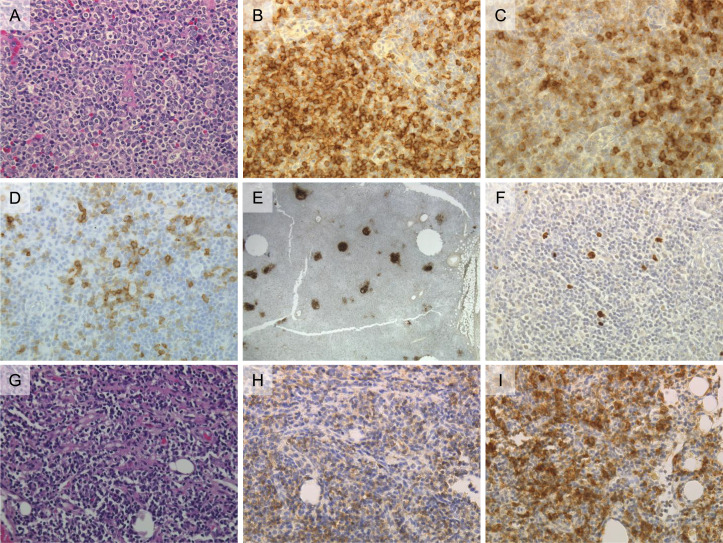
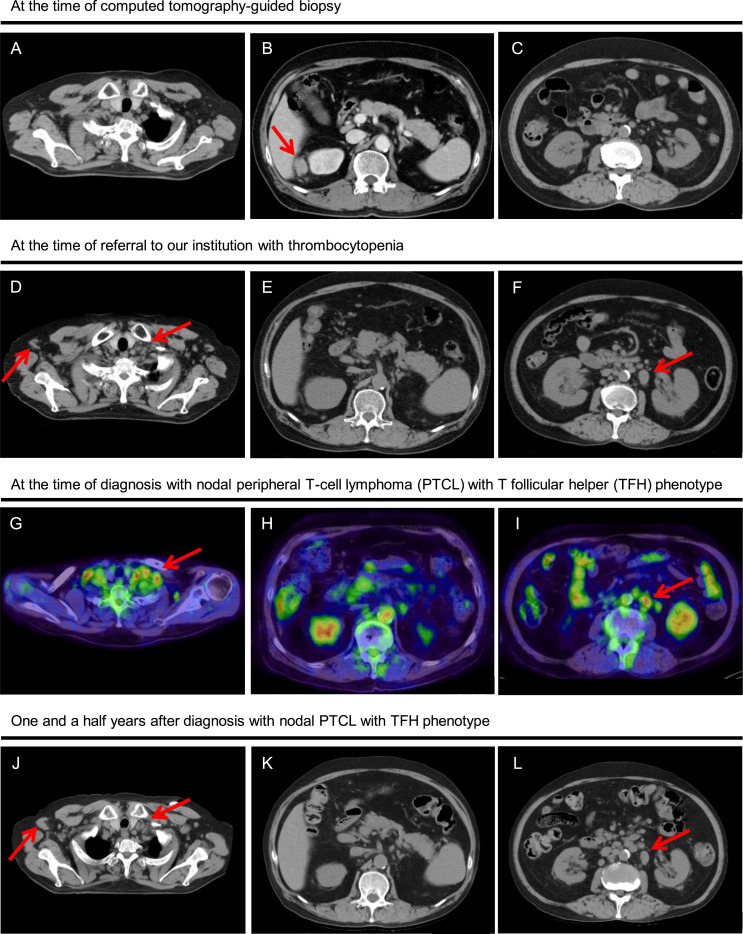
A 71-year-old Japanese man presented with severe thrombocytopenia. A whole-body CT at presentation showed small cervical, axillary, and para-aortic lymphadenopathy, leading to suspicion of immune thrombocytopenia due to lymphoma. Biopsy was difficult to perform because of severe thrombocytopenia. Thus, he received prednisolone (PSL) therapy and his platelet count gradually recovered. Two and a half years after PSL therapy initiation, his cervical lymphadenopathy slightly progressed without other clinical symptoms. Hence, a biopsy from the left cervical lymph node was performed, and he was diagnosed with nodal peripheral T-cell lymphoma (PTCL) with T follicular helper (TFH) phenotype. Due to various complications, we continued treatment with prednisolone alone after the diagnosis of lymphoma; however, there was no further increase in lymph node enlargement and no other lymphoma-related symptoms for one and a half years after diagnosis. Although immunosuppressive therapy has been reported to produce a response in some patients with angioimmunoblastic T-cell lymphoma, our experience suggests that a similar subset may exist in patients with nodal PTCL with TFH phenotype, which has the same cellular origin. Immunosuppressive therapies may constitute an alternative treatment option even in the era of novel molecular-targeted therapies, especially for elderly patients who are ineligible for chemotherapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


