Cumulative Laxation Response with Methylnaltrexone: Implications for Hospitalized Patients with Advanced Illness and Opioid-Induced Constipation
Background
Opioid-induced constipation (OIC) may increase the risk of fecal impaction and mortality in patients with advanced illness. Methylnaltrexone (MNTX) is efficacious for OIC.
Objective
The purpose of this analysis was to evaluate cumulative rescue-free laxation response with repeat MNTX dosing in patients with advanced illness who were refractory to current laxative regimens and to assess the influence, if any, of poor functional status on response to MNTX treatment.
Methods
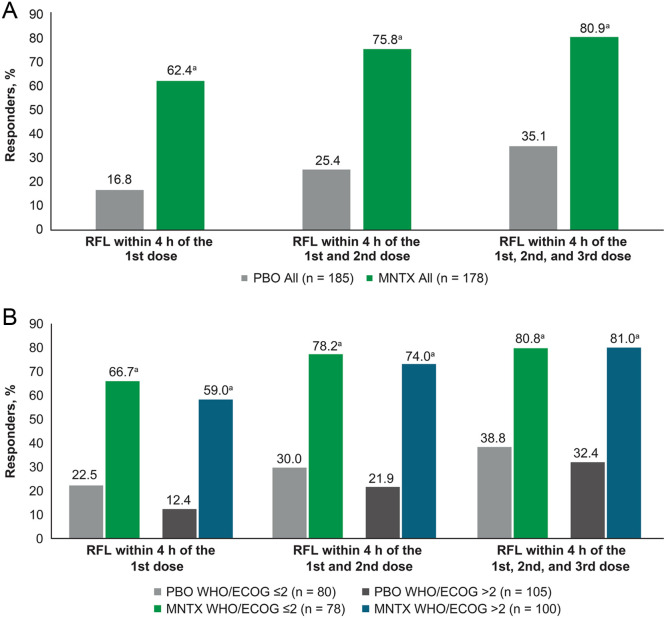
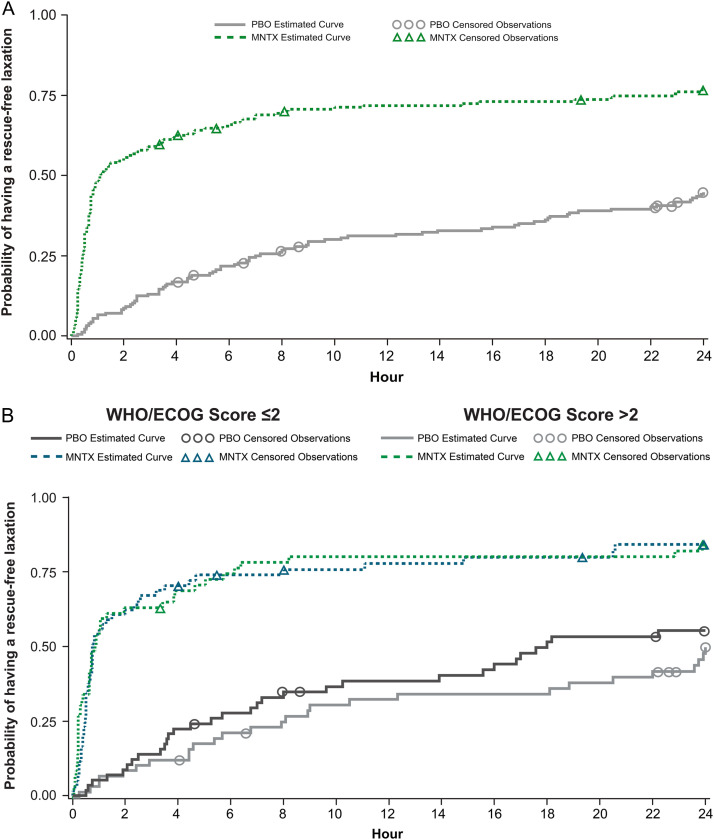
This analysis included pooled data from patients with advanced illness and established OIC who were on a stable opioid regimen in a pivotal, randomized, placebo (PBO)-controlled clinical trial (study 302 [NCT00402038]) or a randomized, PBO-controlled Food and Drug Administration-required postmarketing study (study 4000 [NCT00672477]). Patients in study 302 received subcutaneous MNTX 0.15 mg/kg or PBO every other day, whereas those in study 4000 received MNTX 8 mg (body weight ≥38 to <62 kg), MNTX 12 mg (body weight ≥62 kg), or PBO every other day. Outcomes included cumulative rescue-free laxation rates at 4- and 24-hours postdose for the first 3 doses of study drug and time to rescue-free laxation. To assess if functional status influenced treatment outcomes, we performed a secondary analysis on the outcomes stratified by baseline World Health Organization/Eastern Cooperative Oncology Group performance status, pain scores, and safety.
Results
One hundred eighty-five patients received PBO and 179 patients received MNTX. The median age was 66.0 years, 51.5% were women, 56.5% had a baseline World Health Organization/Eastern Cooperative Oncology Group performance status score >2, and 63.4% had a primary diagnosis of cancer. Cumulative rescue-free laxation rates were significantly higher with MNTX than PBO 4- and 24-hours after doses 1, 2, and 3 (P < 0.0001), and between-treatment comparisons remained significant (P < 0.0001) regardless of performance status. The estimated time to first rescue-free laxation was shorter for patients receiving MNTX versus PBO. No new safety signals were identified.
Conclusions
Repeated use of MNTX represents a safe and effective treatment for OIC in patients with advanced illness regardless of baseline performance status. ClinicalTrials.gov identifier: NCT00672477. (Curr Ther Res Clin Exp. 2023; 84:XXX–XXX)
期刊介绍:
We also encourage the submission of manuscripts presenting preclinical and very preliminary research that may stimulate further investigation of potentially relevant findings, as well as in-depth review articles on specific therapies or disease states, and applied health delivery or pharmacoeconomics.
CTR encourages and supports the submission of manuscripts describing:
• Interventions designed to understand or improve human health, disease treatment or disease prevention;
• Studies that focus on problems that are uncommon in resource-rich countries;
• Research that is "under-published" because of limited access to monetary resources such as English language support and Open Access fees (CTR offers deeply discounted English language editing);
• Republication of articles previously published in non-English journals (eg, evidence-based guidelines) which could be useful if translated into English;
• Preclinical and clinical product development studies that are not pursued for further investigation based upon early phase results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


