Jari Dahmen, Quinten G H Rikken, Gino M M J Kerkhoffs, Sjoerd A S Stufkens
{"title":"距骨髂骨骨膜移植术治疗距骨外侧骨软骨病变:手术技术。","authors":"Jari Dahmen, Quinten G H Rikken, Gino M M J Kerkhoffs, Sjoerd A S Stufkens","doi":"10.1007/s00064-022-00789-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To provide a natural scaffold, good quality cells, and growth factors to facilitate replacement of the complete osteochondral unit with matching talar curvature for large osteochondral lesions of the lateral talar dome.</p><p><strong>Indications: </strong>Symptomatic primary and non-primary lateral osteochondral lesions of the talus not responding to conservative treatment. The anterior-posterior or medial-lateral diameter should exceed 10 mm on computed tomography (CT) for primary lesions; for secondary lesions, there are no size limitations.</p><p><strong>Contraindications: </strong>Tibiotalar osteoarthritis grade III, malignancy, active infectious ankle joint pathology, and hemophilic or other diffuse arthropathy.</p><p><strong>Surgical technique: </strong>Anterolateral arthrotomy is performed after which the Anterior TaloFibular Ligament (ATFL) is disinserted from the fibula. Additional exposure is achieved by placing a Hintermann distractor subluxating the talus ventrally. Thereafter, the osteochondral lesion is excised in toto from the talar dome. The recipient site is micro-drilled in order to disrupt subchondral bone vessels. Thereafter, the autograft is harvested from the ipsilateral iliac crest with an oscillating saw, after which the graft is adjusted to an exactly fitting shape to match the extracted lateral osteochondral defect and the talar morphology as well as curvature. The graft is implanted with a press-fit technique after which the ATFL is re-inserted followed by potential augmentation with an InternalBrace™ (Arthrex, Naples, FL, USA).</p><p><strong>Postoperative management: </strong>Non-weightbearing cast for 6 weeks, followed by another 6 weeks with a walking boot. After 12 weeks, a computed tomography (CT) scan is performed to assess consolidation of the inserted autograft. The patient is referred to a physiotherapist.</p>","PeriodicalId":54677,"journal":{"name":"Operative Orthopadie Und Traumatologie","volume":"35 2","pages":"82-91"},"PeriodicalIF":1.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10076387/pdf/","citationCount":"1","resultStr":"{\"title\":\"Talar OsteoPeriostic grafting from the Iliac Crest (TOPIC) for lateral osteochondral lesions of the talus: operative technique.\",\"authors\":\"Jari Dahmen, Quinten G H Rikken, Gino M M J Kerkhoffs, Sjoerd A S Stufkens\",\"doi\":\"10.1007/s00064-022-00789-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To provide a natural scaffold, good quality cells, and growth factors to facilitate replacement of the complete osteochondral unit with matching talar curvature for large osteochondral lesions of the lateral talar dome.</p><p><strong>Indications: </strong>Symptomatic primary and non-primary lateral osteochondral lesions of the talus not responding to conservative treatment. The anterior-posterior or medial-lateral diameter should exceed 10 mm on computed tomography (CT) for primary lesions; for secondary lesions, there are no size limitations.</p><p><strong>Contraindications: </strong>Tibiotalar osteoarthritis grade III, malignancy, active infectious ankle joint pathology, and hemophilic or other diffuse arthropathy.</p><p><strong>Surgical technique: </strong>Anterolateral arthrotomy is performed after which the Anterior TaloFibular Ligament (ATFL) is disinserted from the fibula. Additional exposure is achieved by placing a Hintermann distractor subluxating the talus ventrally. Thereafter, the osteochondral lesion is excised in toto from the talar dome. The recipient site is micro-drilled in order to disrupt subchondral bone vessels. Thereafter, the autograft is harvested from the ipsilateral iliac crest with an oscillating saw, after which the graft is adjusted to an exactly fitting shape to match the extracted lateral osteochondral defect and the talar morphology as well as curvature. The graft is implanted with a press-fit technique after which the ATFL is re-inserted followed by potential augmentation with an InternalBrace™ (Arthrex, Naples, FL, USA).</p><p><strong>Postoperative management: </strong>Non-weightbearing cast for 6 weeks, followed by another 6 weeks with a walking boot. After 12 weeks, a computed tomography (CT) scan is performed to assess consolidation of the inserted autograft. The patient is referred to a physiotherapist.</p>\",\"PeriodicalId\":54677,\"journal\":{\"name\":\"Operative Orthopadie Und Traumatologie\",\"volume\":\"35 2\",\"pages\":\"82-91\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10076387/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Operative Orthopadie Und Traumatologie\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00064-022-00789-0\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Operative Orthopadie Und Traumatologie","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00064-022-00789-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Talar OsteoPeriostic grafting from the Iliac Crest (TOPIC) for lateral osteochondral lesions of the talus: operative technique.
Objective: To provide a natural scaffold, good quality cells, and growth factors to facilitate replacement of the complete osteochondral unit with matching talar curvature for large osteochondral lesions of the lateral talar dome.
Indications: Symptomatic primary and non-primary lateral osteochondral lesions of the talus not responding to conservative treatment. The anterior-posterior or medial-lateral diameter should exceed 10 mm on computed tomography (CT) for primary lesions; for secondary lesions, there are no size limitations.
Contraindications: Tibiotalar osteoarthritis grade III, malignancy, active infectious ankle joint pathology, and hemophilic or other diffuse arthropathy.
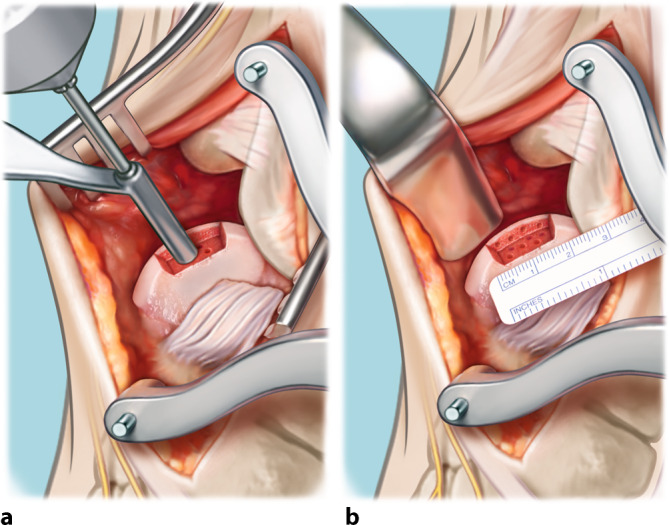
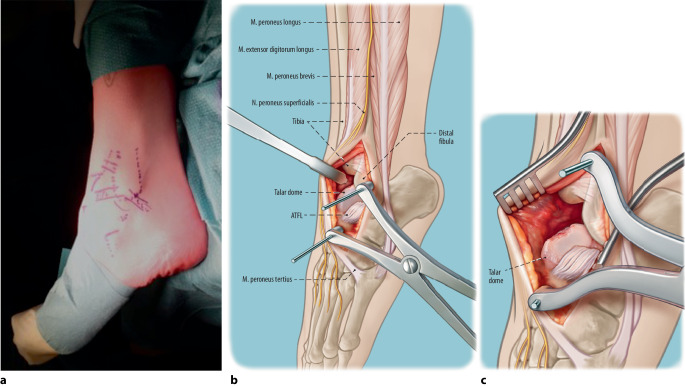
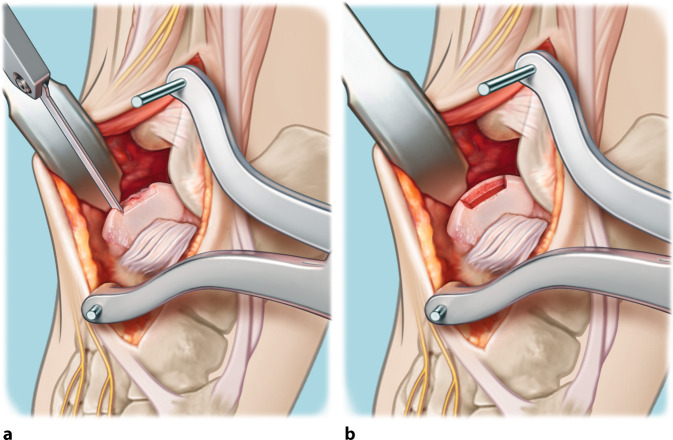
Surgical technique: Anterolateral arthrotomy is performed after which the Anterior TaloFibular Ligament (ATFL) is disinserted from the fibula. Additional exposure is achieved by placing a Hintermann distractor subluxating the talus ventrally. Thereafter, the osteochondral lesion is excised in toto from the talar dome. The recipient site is micro-drilled in order to disrupt subchondral bone vessels. Thereafter, the autograft is harvested from the ipsilateral iliac crest with an oscillating saw, after which the graft is adjusted to an exactly fitting shape to match the extracted lateral osteochondral defect and the talar morphology as well as curvature. The graft is implanted with a press-fit technique after which the ATFL is re-inserted followed by potential augmentation with an InternalBrace™ (Arthrex, Naples, FL, USA).
Postoperative management: Non-weightbearing cast for 6 weeks, followed by another 6 weeks with a walking boot. After 12 weeks, a computed tomography (CT) scan is performed to assess consolidation of the inserted autograft. The patient is referred to a physiotherapist.
期刊介绍:
Orthopedics and Traumatology is directed toward all orthopedic surgeons, trauma-tologists, hand surgeons, specialists in sports injuries, orthopedics and rheumatology as well as gene-al surgeons who require access to reliable information on current operative methods to ensure the quality of patient advice, preoperative planning, and postoperative care.
The journal presents established and new operative procedures in uniformly structured and extensively illustrated contributions. All aspects are presented step-by-step from indications, contraindications, patient education, and preparation of the operation right through to postoperative care. The advantages and disadvantages, possible complications, deficiencies and risks of the methods as well as significant results with their evaluation criteria are discussed. To allow the reader to assess the outcome, results are detailed and based on internationally recognized scoring systems.
Orthopedics and Traumatology facilitates effective advancement and further education for all those active in both special and conservative fields of orthopedics, traumatology, and general surgery, offers sup-port for therapeutic decision-making, and provides – more than 30 years after its first publication – constantly expanding and up-to-date teaching on operative techniques.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


