Silvan Licher, Frank J Wolters, Jelena Pavlović, Maryam Kavousi, Maarten J G Leening, M Kamran Ikram, M Arfan Ikram
{"title":"资格标准对患者选择的影响以及 10 项多领域痴呆症预防试验的治疗意义:基于人群的研究","authors":"Silvan Licher, Frank J Wolters, Jelena Pavlović, Maryam Kavousi, Maarten J G Leening, M Kamran Ikram, M Arfan Ikram","doi":"10.1159/000528120","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Dementia prevention trials have so far shown little benefit of multidomain interventions against cognitive decline. Recruitment strategies in these trials often centre around dementia risk or cardiovascular risk profile, but it is uncertain whether this leads to inclusion of individuals who may benefit most from the intervention. We determined the effects of eligibility criteria on the recruitment of potential trial participants in the general population.</p><p><strong>Methods: </strong>In a systematic search until January 1, 2022, we identified all published and ongoing large (≥500 participants), phase-3 multidomain trials for the prevention of cognitive decline or dementia. We applied trial eligibility criteria to 5,381 participants of the population-based Rotterdam Study (mean age: 72 years, 58% women), to compare participant characteristics, predicted risk of cardiovascular disease, and dementia risk, between trial eligible and ineligible persons.</p><p><strong>Results: </strong>We identified 10 trials, of which 5 had been published (DR's EXTRA, FINGER, preDIVA, MAPT, and HATICE) and 5 are ongoing (US-POINTER, MIND-CHINA, MYB, AgeWell.de, and J-Mint). Among all Rotterdam Study participants, eligibility across published trials ranged from 48% for MAPT to 87% for preDIVA, in line with original trial reports. Variability in eligibility was wider for ongoing trials, from 1% for US-POINTER to over 94% for MYB trial. Over 70% of trial eligible individuals are recommended preventive intervention in routine care based on their cardiovascular risk, similar for lipid-lowering (71%) and blood pressure-lowering treatment (73%). Ten-year risks of dementia were similar for eligible compared to ineligible individuals (12 vs. 11%).</p><p><strong>Conclusion: </strong>Multidomain dementia prevention trials fail to preferentially include those at the highest risk of dementia and mostly include individuals who qualify for interventions already on the basis of cardiovascular prevention guidelines. These findings call for better targeted enrolment of individuals for whom trial results can improve clinical decision-making.</p>","PeriodicalId":54730,"journal":{"name":"Neuroepidemiology","volume":"57 1","pages":"14-24"},"PeriodicalIF":3.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10064383/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of Eligibility Criteria on Patient Selection and Treatment Implications from 10 Multidomain Dementia Prevention Trials: A Population-Based Study.\",\"authors\":\"Silvan Licher, Frank J Wolters, Jelena Pavlović, Maryam Kavousi, Maarten J G Leening, M Kamran Ikram, M Arfan Ikram\",\"doi\":\"10.1159/000528120\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Dementia prevention trials have so far shown little benefit of multidomain interventions against cognitive decline. Recruitment strategies in these trials often centre around dementia risk or cardiovascular risk profile, but it is uncertain whether this leads to inclusion of individuals who may benefit most from the intervention. We determined the effects of eligibility criteria on the recruitment of potential trial participants in the general population.</p><p><strong>Methods: </strong>In a systematic search until January 1, 2022, we identified all published and ongoing large (≥500 participants), phase-3 multidomain trials for the prevention of cognitive decline or dementia. We applied trial eligibility criteria to 5,381 participants of the population-based Rotterdam Study (mean age: 72 years, 58% women), to compare participant characteristics, predicted risk of cardiovascular disease, and dementia risk, between trial eligible and ineligible persons.</p><p><strong>Results: </strong>We identified 10 trials, of which 5 had been published (DR's EXTRA, FINGER, preDIVA, MAPT, and HATICE) and 5 are ongoing (US-POINTER, MIND-CHINA, MYB, AgeWell.de, and J-Mint). Among all Rotterdam Study participants, eligibility across published trials ranged from 48% for MAPT to 87% for preDIVA, in line with original trial reports. Variability in eligibility was wider for ongoing trials, from 1% for US-POINTER to over 94% for MYB trial. Over 70% of trial eligible individuals are recommended preventive intervention in routine care based on their cardiovascular risk, similar for lipid-lowering (71%) and blood pressure-lowering treatment (73%). Ten-year risks of dementia were similar for eligible compared to ineligible individuals (12 vs. 11%).</p><p><strong>Conclusion: </strong>Multidomain dementia prevention trials fail to preferentially include those at the highest risk of dementia and mostly include individuals who qualify for interventions already on the basis of cardiovascular prevention guidelines. These findings call for better targeted enrolment of individuals for whom trial results can improve clinical decision-making.</p>\",\"PeriodicalId\":54730,\"journal\":{\"name\":\"Neuroepidemiology\",\"volume\":\"57 1\",\"pages\":\"14-24\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10064383/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neuroepidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000528120\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/11/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuroepidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000528120","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Effects of Eligibility Criteria on Patient Selection and Treatment Implications from 10 Multidomain Dementia Prevention Trials: A Population-Based Study.
Introduction: Dementia prevention trials have so far shown little benefit of multidomain interventions against cognitive decline. Recruitment strategies in these trials often centre around dementia risk or cardiovascular risk profile, but it is uncertain whether this leads to inclusion of individuals who may benefit most from the intervention. We determined the effects of eligibility criteria on the recruitment of potential trial participants in the general population.
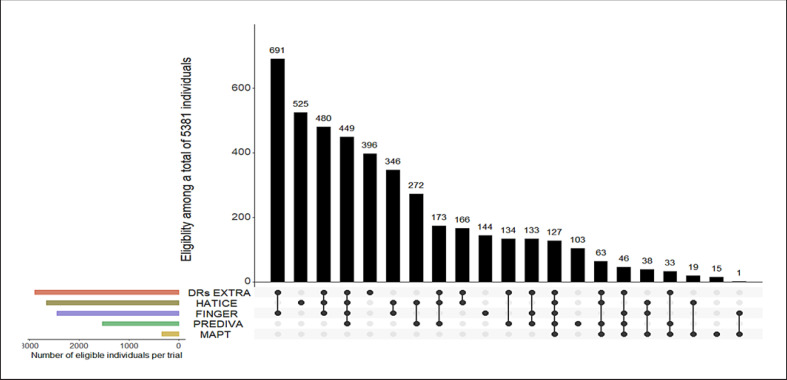
Methods: In a systematic search until January 1, 2022, we identified all published and ongoing large (≥500 participants), phase-3 multidomain trials for the prevention of cognitive decline or dementia. We applied trial eligibility criteria to 5,381 participants of the population-based Rotterdam Study (mean age: 72 years, 58% women), to compare participant characteristics, predicted risk of cardiovascular disease, and dementia risk, between trial eligible and ineligible persons.
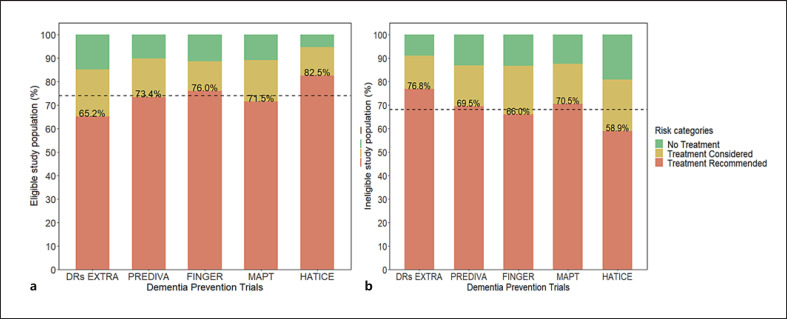
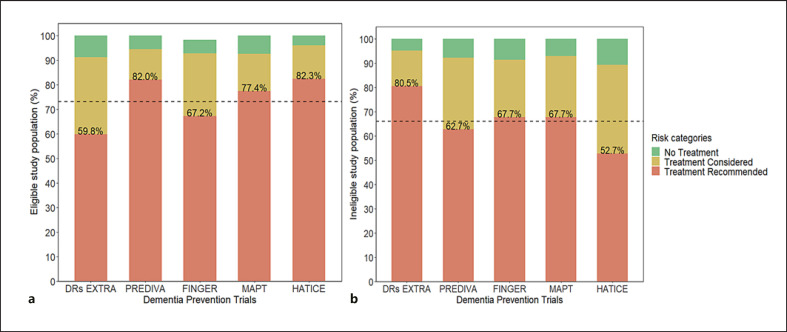
Results: We identified 10 trials, of which 5 had been published (DR's EXTRA, FINGER, preDIVA, MAPT, and HATICE) and 5 are ongoing (US-POINTER, MIND-CHINA, MYB, AgeWell.de, and J-Mint). Among all Rotterdam Study participants, eligibility across published trials ranged from 48% for MAPT to 87% for preDIVA, in line with original trial reports. Variability in eligibility was wider for ongoing trials, from 1% for US-POINTER to over 94% for MYB trial. Over 70% of trial eligible individuals are recommended preventive intervention in routine care based on their cardiovascular risk, similar for lipid-lowering (71%) and blood pressure-lowering treatment (73%). Ten-year risks of dementia were similar for eligible compared to ineligible individuals (12 vs. 11%).
Conclusion: Multidomain dementia prevention trials fail to preferentially include those at the highest risk of dementia and mostly include individuals who qualify for interventions already on the basis of cardiovascular prevention guidelines. These findings call for better targeted enrolment of individuals for whom trial results can improve clinical decision-making.
期刊介绍:
''Neuroepidemiology'' is the only internationally recognised peer-reviewed periodical devoted to descriptive, analytical and experimental studies in the epidemiology of neurologic disease. The scope of the journal expands the boundaries of traditional clinical neurology by providing new insights regarding the etiology, determinants, distribution, management and prevention of diseases of the nervous system.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


