调整基于证据的预防跌倒计划以实现远程交付--通过 RE-AIM 评估框架促进健康公平的实施启示。
摘要
由于老年人死亡和住院的风险较高,COVID-19 对老年人的健康和福祉造成了极大的影响,其中许多老年人患有慢性疾病。它还造成了一些次要的流行病,包括跌倒风险增加、久坐不动、社会隔离以及由于封锁政策造成的行动受限而缺乏运动。跌倒是导致可预防的死亡和住院的主要原因,因此,亲自参与的循证跌倒预防计划(EBFPPs)必须转向远程实施。2020 年春季,许多 EBFPP 管理员开始重新设计远程交付计划,以适应大流行病所需的物理距离准则。对于老年人和残疾人来说,向远程交付过渡至关重要,这样他们就可以利用 EBFPP 保持健康、不跌倒、不受伤、不住院,并保持社交活动。我们与社区生活管理局 (ACL)、国家老龄化委员会 (NCOA) 和国家预防跌倒资源中心 (NFPRC) 合作,对远程提供的 EBFPPs 进行了深入的实施评估。我们研究了调整和实施远程交付的四个 EBFPP 的过程,以及在 RE-AIM 评估框架内远程实施项目的最佳实践。这加强了 NFPRC 正在进行的支持 EBFPPs 传播、实施和可持续性的工作。我们有目的性地对组织进行了抽样调查,以最大限度地反映组织和提供者类型、地理位置以及服务不足的老年人群(黑人、土著或其他有色人种 (BIPOC)、农村、残疾)的差异。该定性评估包括与项目管理人员、员工和领导进行的半结构化访谈(N = 22)中提供的服务提供者层面的数据。访谈指南包括使用 Wiltsey-Stirman (2019) 适应性框架 (FRAME),对 EBFPP 干预和实施策略进行调整的内容、原因和方式、覆盖范围和实施结果(可接受性、可行性、忠实性和成本;Proctor 等人,2011 年),重点关注公平性,以了解这些项目为谁工作以及解决不公平问题的机会。研究结果表明,远程 EBFPP 与研究人员和社区组织合作,对远程交付进行了有计划且忠实度一致的调整,重点关注项目内容和交付中参与者的安全。交付地点和领导者需要使用和访问技术的支持,以促进参与,并随着时间的推移不断改进。虽然从项目管理人员、领导者和工作人员的角度来看,远程提供 EBFPP 增加了某些人群(如照顾者、农村居民、身体残疾者)参与 EBFPP 的机会,但数字鸿沟仍然是获得和舒适使用技术的障碍。远程交付的 EBFPP 对于交付机构和领导者来说是可接受的、可行的,并且能够通过项目开发者的改编忠实地交付,但与面对面相比,远程交付的 EBFPP 需要更多的资源,实施成本也更高。这项工作在大流行病之外也有重要意义。远程授课扩大了传统上无法获得面授课程服务的群体,尤其是残疾人群体。这项工作将有助于回答以下重要问题:对于有跌倒风险的老年人和残障人士、慢性病患者以及在获得医疗保健、健康促进计划和健康结果方面最容易出现差异的社区而言,计划实施的覆盖范围、可及性、可行性和成本。它还将为资助者提供重要信息,使其了解将已证明在现场环境中有效的 EBFPP 项目改编为远程交付所需的要素,以达到可比的效果。
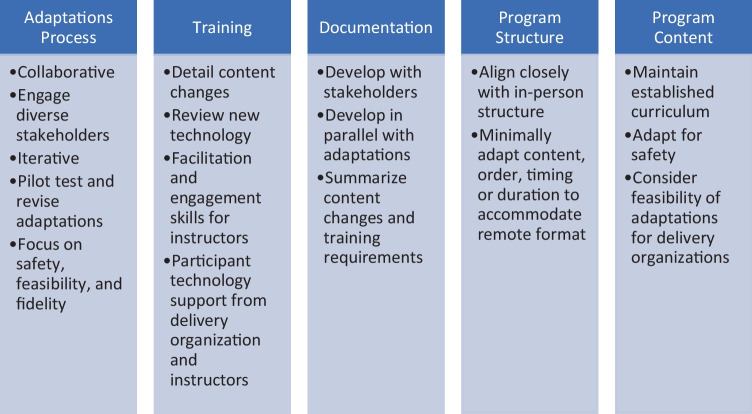
COVID-19 disproportionally impacted the health and well-being of older adults-many of whom live with chronic conditions-due to their higher risk of dying and being hospitalized. It also created several secondary pandemics, including increased falls risk, sedentary behavior, social isolation, and physical inactivity due to limitations in mobility from lock-down policies. With falls as the leading cause of preventable death and hospitalizations, it became vital for in-person evidence-based falls prevention programs (EBFPPs) to pivot to remote delivery. In Spring 2020, many EBFPP administrators began re-designing programs for remote delivery to accommodate physical distancing guidelines necessitated by the pandemic. Transition to remote delivery was essential for older adults and persons with disabilities to access EBFPPs for staying healthy, falls and injury free, out of hospitals, and also keeping them socially engaged. We collaborated with the Administration on Community Living (ACL), the National Council on Aging (NCOA), and the National Falls Prevention Resource Center (NFPRC), for an in-depth implementation evaluation of remotely delivered EBFPPs. We examined the process of adapting and implementing four EBFPPs for remote delivery, best practices for implementing the programs remotely within the RE-AIM evaluation framework. This enhances NFPRC's ongoing work supporting dissemination, implementation, and sustainability of EBFPPs. We purposively sampled organizations for maximum variation in organization and provider type, geographic location, and reach of underserved older populations (Black, Indigenous, or other People of Color (BIPOC), rural, disabilities). This qualitative evaluation includes provider-level data from semi-structured interviews (N = 22) with program administrators, staff, and leaders. The interview guide included what, why, and how adaptations were made to EBFPP interventions and implementation strategies using Wiltsey-Stirman (2019) adaptations framework (FRAME), reach, and implementation outcomes (acceptability, feasibility, fidelity, and costs; Proctor et al., 2011), focusing on equity to learn for whom these programs were working and opportunities to address inequities. Findings demonstrate remote EBFPPs made planned and fidelity-consistent adaptations to remote delivery in partnership with researchers and community organizations, focusing on participant safety both in program content and delivery. Supports using and accessing technology were needed for delivery sites and leaders to facilitate engagement, and improved over time. While remote EBFPP delivery has increased access to EBFPPs for some populations from the perspective of program administrator, leaders, and staff (e.g., caregivers, rural-dwellers, persons with physical disabilities), the digital divide remains a barrier in access to and comfort using technology. Remote-delivered EBFPPs were acceptable and feasible to delivery organizations and leaders, were able to be delivered with fidelity using adaptations from program developers, but were more resource intensive and costly to implement compared to in-person. This work has important implications beyond the pandemic. Remote delivery has expanded access to groups traditionally underserved by in-person programming, particularly disability communities. This work will help answer important questions about reach, accessibility, feasibility, and cost of program delivery for older adults and people with disabilities at risk for falls, those living with chronic conditions, and communities most vulnerable to disparities in access to health care, health promotion programming, and health outcomes. It will also provide critical information to funders about elements required to adapt EBFPPs proven effective in in-person settings for remote delivery with fidelity to achieve comparable outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


