Casper Falster, Gro Egholm, Rune Wiig, Mikael Kjær Poulsen, Jacob Eifer Møller, Stefan Posth, Mikkel Brabrand, Christian Borbjerg Laursen
{"title":"定制多器官超声入路诊断疑似肺栓塞的准确性。","authors":"Casper Falster, Gro Egholm, Rune Wiig, Mikael Kjær Poulsen, Jacob Eifer Møller, Stefan Posth, Mikkel Brabrand, Christian Borbjerg Laursen","doi":"10.1055/a-1971-7454","DOIUrl":null,"url":null,"abstract":"<p><p><b>Purpose</b> The aims of this study were to prospectively assess the diagnostic accuracy of a bespoke multiorgan point-of-care ultrasound approach for suspected pulmonary embolism and evaluate if this model allows reduced referral to further radiation diagnostics while maintaining safety standards. <b>Materials and Methods</b> Patients with suspected pulmonary embolism referred for CT pulmonary angiography or ventilation/perfusion scintigraphy were included as a convenience sample. All patients were subject to blinded ultrasound investigation with cardiac, lung, and deep venous ultrasound. The sensitivity and specificity of applied ultrasound signs and the hypothetical reduction in the need for further diagnostic workup were calculated. <b>Results</b> 75 patients were prospectively enrolled. The Wells score was below 2 in 48 patients, between 2 and 6 in 24 patients, and above 6 in 3 patients. The prevalence of pulmonary embolism was 28%. The most notable ultrasound signs were presence of a deep venous thrombus, at least two hypoechoic pleural-based lesions, the D-sign, the 60/60-sign, and a visible right ventricular thrombus which all had a specificity of 100%. Additionally, a multiorgan ultrasound investigation with no findings compatible with pulmonary embolism yielded a sensitivity of 95.2% (95%CI: 76.2-99.9). CT or scintigraphy could be safely avoided in 70% of cases (95%CI: 63.0-83.1%). <b>Conclusion</b> The findings of our study suggest that implementation of a multiorgan ultrasound assessment in patients with suspected pulmonary embolism may safely reduce the need for CT or scintigraphy by confirming or dismissing the suspicion.</p>","PeriodicalId":44852,"journal":{"name":"Ultrasound International Open","volume":"8 2","pages":"E59-E67"},"PeriodicalIF":1.6000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/5e/10-1055-a-1971-7454.PMC9886498.pdf","citationCount":"1","resultStr":"{\"title\":\"Diagnostic Accuracy of a Bespoke Multiorgan Ultrasound Approach in Suspected Pulmonary Embolism.\",\"authors\":\"Casper Falster, Gro Egholm, Rune Wiig, Mikael Kjær Poulsen, Jacob Eifer Møller, Stefan Posth, Mikkel Brabrand, Christian Borbjerg Laursen\",\"doi\":\"10.1055/a-1971-7454\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Purpose</b> The aims of this study were to prospectively assess the diagnostic accuracy of a bespoke multiorgan point-of-care ultrasound approach for suspected pulmonary embolism and evaluate if this model allows reduced referral to further radiation diagnostics while maintaining safety standards. <b>Materials and Methods</b> Patients with suspected pulmonary embolism referred for CT pulmonary angiography or ventilation/perfusion scintigraphy were included as a convenience sample. All patients were subject to blinded ultrasound investigation with cardiac, lung, and deep venous ultrasound. The sensitivity and specificity of applied ultrasound signs and the hypothetical reduction in the need for further diagnostic workup were calculated. <b>Results</b> 75 patients were prospectively enrolled. The Wells score was below 2 in 48 patients, between 2 and 6 in 24 patients, and above 6 in 3 patients. The prevalence of pulmonary embolism was 28%. The most notable ultrasound signs were presence of a deep venous thrombus, at least two hypoechoic pleural-based lesions, the D-sign, the 60/60-sign, and a visible right ventricular thrombus which all had a specificity of 100%. Additionally, a multiorgan ultrasound investigation with no findings compatible with pulmonary embolism yielded a sensitivity of 95.2% (95%CI: 76.2-99.9). CT or scintigraphy could be safely avoided in 70% of cases (95%CI: 63.0-83.1%). <b>Conclusion</b> The findings of our study suggest that implementation of a multiorgan ultrasound assessment in patients with suspected pulmonary embolism may safely reduce the need for CT or scintigraphy by confirming or dismissing the suspicion.</p>\",\"PeriodicalId\":44852,\"journal\":{\"name\":\"Ultrasound International Open\",\"volume\":\"8 2\",\"pages\":\"E59-E67\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2022-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/5e/10-1055-a-1971-7454.PMC9886498.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ultrasound International Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-1971-7454\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-1971-7454","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Diagnostic Accuracy of a Bespoke Multiorgan Ultrasound Approach in Suspected Pulmonary Embolism.
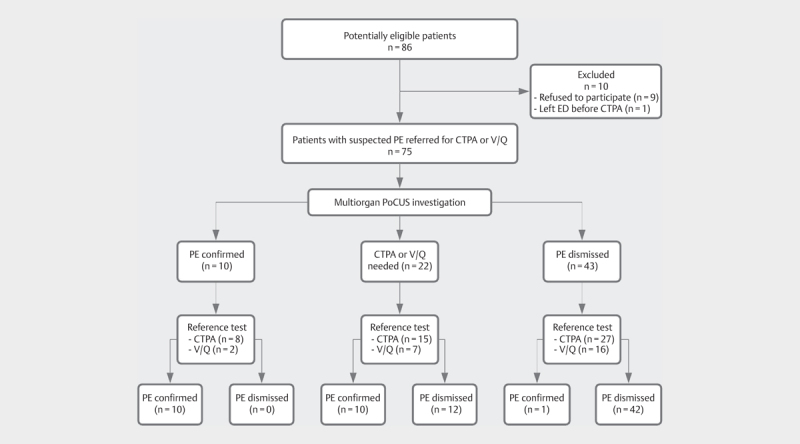
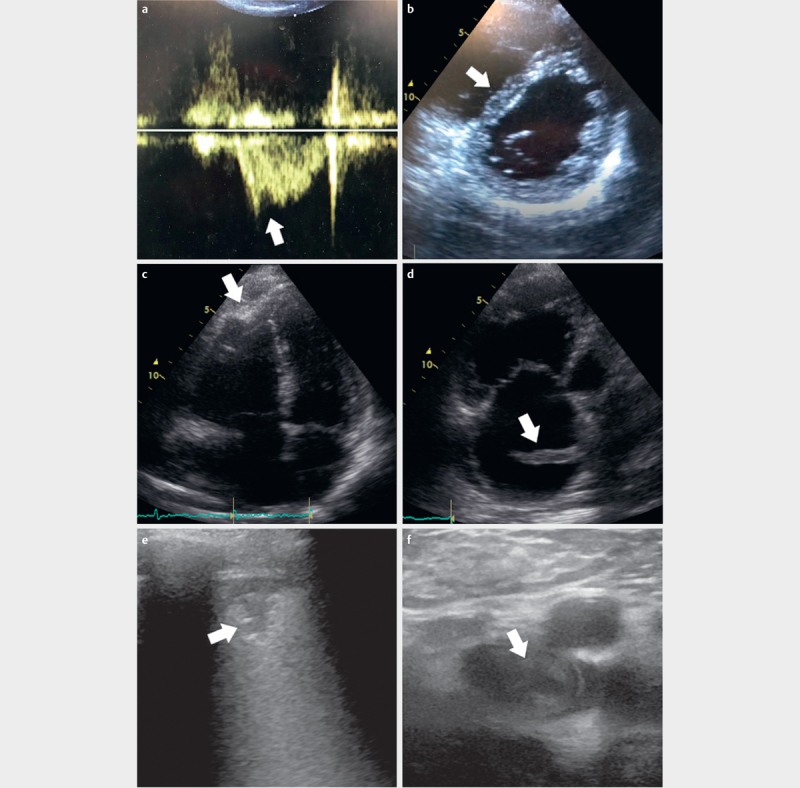
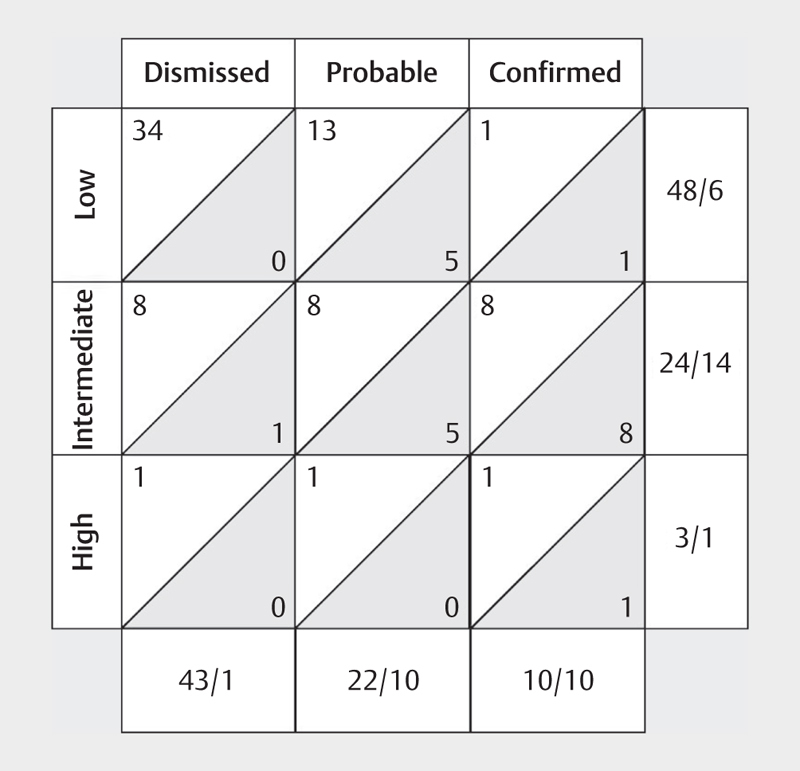
Purpose The aims of this study were to prospectively assess the diagnostic accuracy of a bespoke multiorgan point-of-care ultrasound approach for suspected pulmonary embolism and evaluate if this model allows reduced referral to further radiation diagnostics while maintaining safety standards. Materials and Methods Patients with suspected pulmonary embolism referred for CT pulmonary angiography or ventilation/perfusion scintigraphy were included as a convenience sample. All patients were subject to blinded ultrasound investigation with cardiac, lung, and deep venous ultrasound. The sensitivity and specificity of applied ultrasound signs and the hypothetical reduction in the need for further diagnostic workup were calculated. Results 75 patients were prospectively enrolled. The Wells score was below 2 in 48 patients, between 2 and 6 in 24 patients, and above 6 in 3 patients. The prevalence of pulmonary embolism was 28%. The most notable ultrasound signs were presence of a deep venous thrombus, at least two hypoechoic pleural-based lesions, the D-sign, the 60/60-sign, and a visible right ventricular thrombus which all had a specificity of 100%. Additionally, a multiorgan ultrasound investigation with no findings compatible with pulmonary embolism yielded a sensitivity of 95.2% (95%CI: 76.2-99.9). CT or scintigraphy could be safely avoided in 70% of cases (95%CI: 63.0-83.1%). Conclusion The findings of our study suggest that implementation of a multiorgan ultrasound assessment in patients with suspected pulmonary embolism may safely reduce the need for CT or scintigraphy by confirming or dismissing the suspicion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


