Ruan Spies, Charlotte Schutz, Amy Ward, Avuyonke Balfour, Muki Shey, Mark Nicol, Rosie Burton, Bianca Sossen, Robert Wilkinson, David Barr, Graeme Meintjes
{"title":"艾滋病毒相关结核病住院患者的利福平耐药性和死亡率","authors":"Ruan Spies, Charlotte Schutz, Amy Ward, Avuyonke Balfour, Muki Shey, Mark Nicol, Rosie Burton, Bianca Sossen, Robert Wilkinson, David Barr, Graeme Meintjes","doi":"10.4102/sajhivmed.v23i1.1396","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with HIV and drug-resistant tuberculosis (TB) are at high risk of death.</p><p><strong>Objectives: </strong>We investigated the association between rifampicin-resistant TB (RR-TB) and mortality in a cohort of patients who were admitted to hospital at the time of TB diagnosis.</p><p><strong>Method: </strong>Adults hospitalised at Khayelitsha Hospital and diagnosed with HIV-associated TB during admission, were enrolled between 2013 and 2016. Clinical, biochemical and microbiological data were prospectively collected and participants were followed up for 12 weeks.</p><p><strong>Results: </strong>Participants with microbiologically confirmed TB (<i>n</i> = 482) were enrolled a median of two days (interquartile range [IQR]: 1-3 days) following admission. Fifty-three participants (11.0%) had RR-TB. Participants with rifampicin-susceptible TB (RS-TB) received appropriate treatment a median of one day (IQR: 1-2 days) following enrolment compared to three days (IQR: 1-9 days) in participants with RR-TB. Eight participants with RS-TB (1.9%) and six participants with RR-TB (11.3%) died prior to the initiation of appropriate treatment. Mortality at 12 weeks was 87/429 (20.3%) in the RS-TB group and 21/53 (39.6%) in the RR-TB group. RR-TB was a significant predictor of 12-week mortality (hazard ratio: 1.88; 95% confidence interval: 1.07-3.29; <i>P</i> = 0.03).</p><p><strong>Conclusion: </strong>Mortality at 12 weeks in participants with RR-TB was high compared to participants with RS-TB. Delays in the initiation of appropriate treatment and poorer regimen efficacy are proposed as contributors to higher mortality in hospitalised patients with HIV and RR-TB.</p>","PeriodicalId":49489,"journal":{"name":"Southern African Journal of Hiv Medicine","volume":"23 1","pages":"1396"},"PeriodicalIF":1.6000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9575347/pdf/","citationCount":"0","resultStr":"{\"title\":\"Rifampicin resistance and mortality in patients hospitalised with HIV-associated tuberculosis.\",\"authors\":\"Ruan Spies, Charlotte Schutz, Amy Ward, Avuyonke Balfour, Muki Shey, Mark Nicol, Rosie Burton, Bianca Sossen, Robert Wilkinson, David Barr, Graeme Meintjes\",\"doi\":\"10.4102/sajhivmed.v23i1.1396\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with HIV and drug-resistant tuberculosis (TB) are at high risk of death.</p><p><strong>Objectives: </strong>We investigated the association between rifampicin-resistant TB (RR-TB) and mortality in a cohort of patients who were admitted to hospital at the time of TB diagnosis.</p><p><strong>Method: </strong>Adults hospitalised at Khayelitsha Hospital and diagnosed with HIV-associated TB during admission, were enrolled between 2013 and 2016. Clinical, biochemical and microbiological data were prospectively collected and participants were followed up for 12 weeks.</p><p><strong>Results: </strong>Participants with microbiologically confirmed TB (<i>n</i> = 482) were enrolled a median of two days (interquartile range [IQR]: 1-3 days) following admission. Fifty-three participants (11.0%) had RR-TB. Participants with rifampicin-susceptible TB (RS-TB) received appropriate treatment a median of one day (IQR: 1-2 days) following enrolment compared to three days (IQR: 1-9 days) in participants with RR-TB. Eight participants with RS-TB (1.9%) and six participants with RR-TB (11.3%) died prior to the initiation of appropriate treatment. Mortality at 12 weeks was 87/429 (20.3%) in the RS-TB group and 21/53 (39.6%) in the RR-TB group. RR-TB was a significant predictor of 12-week mortality (hazard ratio: 1.88; 95% confidence interval: 1.07-3.29; <i>P</i> = 0.03).</p><p><strong>Conclusion: </strong>Mortality at 12 weeks in participants with RR-TB was high compared to participants with RS-TB. Delays in the initiation of appropriate treatment and poorer regimen efficacy are proposed as contributors to higher mortality in hospitalised patients with HIV and RR-TB.</p>\",\"PeriodicalId\":49489,\"journal\":{\"name\":\"Southern African Journal of Hiv Medicine\",\"volume\":\"23 1\",\"pages\":\"1396\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9575347/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Southern African Journal of Hiv Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4102/sajhivmed.v23i1.1396\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Southern African Journal of Hiv Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4102/sajhivmed.v23i1.1396","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Rifampicin resistance and mortality in patients hospitalised with HIV-associated tuberculosis.
Background: Patients with HIV and drug-resistant tuberculosis (TB) are at high risk of death.
Objectives: We investigated the association between rifampicin-resistant TB (RR-TB) and mortality in a cohort of patients who were admitted to hospital at the time of TB diagnosis.
Method: Adults hospitalised at Khayelitsha Hospital and diagnosed with HIV-associated TB during admission, were enrolled between 2013 and 2016. Clinical, biochemical and microbiological data were prospectively collected and participants were followed up for 12 weeks.
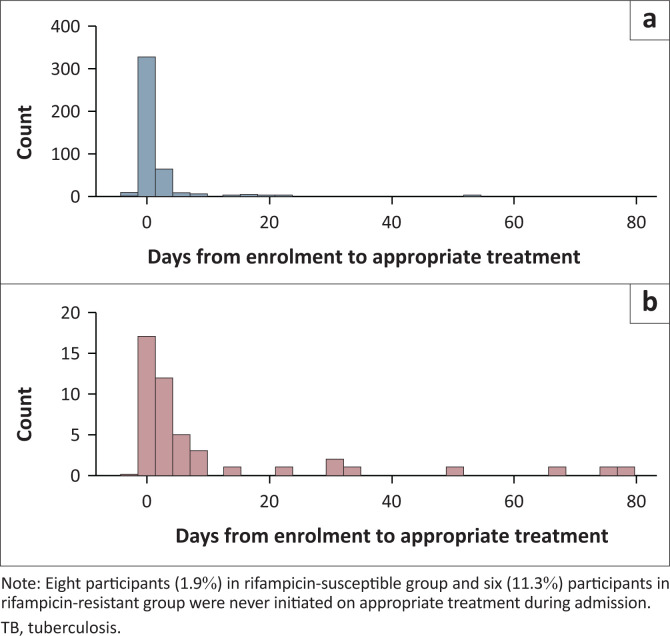
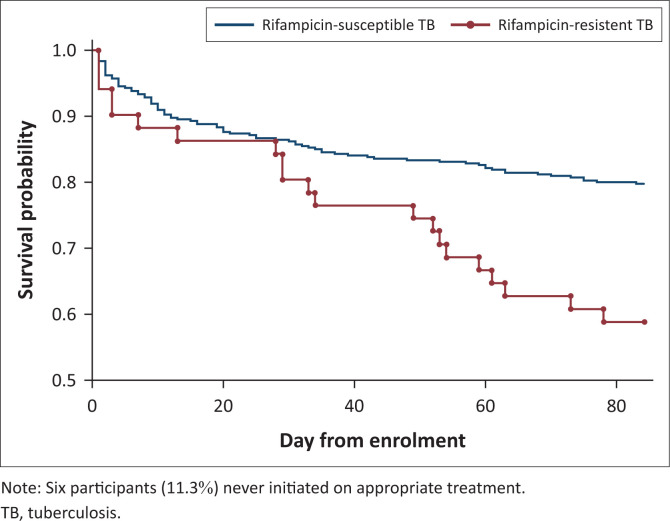
Results: Participants with microbiologically confirmed TB (n = 482) were enrolled a median of two days (interquartile range [IQR]: 1-3 days) following admission. Fifty-three participants (11.0%) had RR-TB. Participants with rifampicin-susceptible TB (RS-TB) received appropriate treatment a median of one day (IQR: 1-2 days) following enrolment compared to three days (IQR: 1-9 days) in participants with RR-TB. Eight participants with RS-TB (1.9%) and six participants with RR-TB (11.3%) died prior to the initiation of appropriate treatment. Mortality at 12 weeks was 87/429 (20.3%) in the RS-TB group and 21/53 (39.6%) in the RR-TB group. RR-TB was a significant predictor of 12-week mortality (hazard ratio: 1.88; 95% confidence interval: 1.07-3.29; P = 0.03).
Conclusion: Mortality at 12 weeks in participants with RR-TB was high compared to participants with RS-TB. Delays in the initiation of appropriate treatment and poorer regimen efficacy are proposed as contributors to higher mortality in hospitalised patients with HIV and RR-TB.
期刊介绍:
The Southern African Journal of HIV Medicine is focused on HIV/AIDS treatment, prevention and related topics relevant to clinical and public health practice. The purpose of the journal is to disseminate original research results and to support high-level learning related to HIV Medicine. It publishes original research articles, editorials, case reports/case series, reviews of state-of-the-art clinical practice, and correspondence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


