Kana Fukui, Shoichiro Amari, Nobuyuki Yotani, Rika Kosaki, Kenichiro Hata, Motomichi Kosuga, Haruhiko Sago, Tetsuya Isayama, Yushi Ito
{"title":"新生儿粘多糖病伴顽固性腹水1例。","authors":"Kana Fukui, Shoichiro Amari, Nobuyuki Yotani, Rika Kosaki, Kenichiro Hata, Motomichi Kosuga, Haruhiko Sago, Tetsuya Isayama, Yushi Ito","doi":"10.1055/a-2028-7784","DOIUrl":null,"url":null,"abstract":"<p><p>We report a case of a patient with severe fetal hydrops and refractory ascites, diagnosed as mucopolysaccharidosis type VII (MPS VII) by whole-exome sequencing, and discharged at 5 months of age after long-term ventilatory management. A male neonate was born by emergency cesarean section due to fetal distress at 30 <sup>1/7</sup> weeks' gestation. Physical examination and X-rays revealed pleural effusion, ascites, and generalized edema, indicating severe fetal hydrops. He underwent tracheal intubation because of respiratory distress that was attributed to massive ascites, pulmonary hypoplasia, and pulmonary hypertension. He received mechanical ventilation and inhaled nitric oxide therapy. Prednisone, octreotide, and a factor XIII preparation were used as the treatment for ascites, and the ascites gradually decreased. He was extubated within 2 months of age. At 4 months of age, the results of whole-exome sequencing of the cord blood showed a compound heterozygous mutation in the <i>GUSB</i> gene, the gene responsible for MPS VII. Enzyme replacement therapy was initiated, and the ascites was resolved. Careful systemic management, including lung-protective respiratory management and the early establishment of nutrition, is important for the long-term survival of infants with fetal hydrops, and early aggressive workup, including whole-genome sequencing for the cause, should be performed in the case of refractory ascites.</p>","PeriodicalId":7645,"journal":{"name":"AJP Reports","volume":"13 1","pages":"e25-e28"},"PeriodicalIF":0.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/da/a1/10-1055-a-2028-7784.PMC10019997.pdf","citationCount":"0","resultStr":"{\"title\":\"A Neonate with Mucopolysaccharidosis Type VII with Intractable Ascites.\",\"authors\":\"Kana Fukui, Shoichiro Amari, Nobuyuki Yotani, Rika Kosaki, Kenichiro Hata, Motomichi Kosuga, Haruhiko Sago, Tetsuya Isayama, Yushi Ito\",\"doi\":\"10.1055/a-2028-7784\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We report a case of a patient with severe fetal hydrops and refractory ascites, diagnosed as mucopolysaccharidosis type VII (MPS VII) by whole-exome sequencing, and discharged at 5 months of age after long-term ventilatory management. A male neonate was born by emergency cesarean section due to fetal distress at 30 <sup>1/7</sup> weeks' gestation. Physical examination and X-rays revealed pleural effusion, ascites, and generalized edema, indicating severe fetal hydrops. He underwent tracheal intubation because of respiratory distress that was attributed to massive ascites, pulmonary hypoplasia, and pulmonary hypertension. He received mechanical ventilation and inhaled nitric oxide therapy. Prednisone, octreotide, and a factor XIII preparation were used as the treatment for ascites, and the ascites gradually decreased. He was extubated within 2 months of age. At 4 months of age, the results of whole-exome sequencing of the cord blood showed a compound heterozygous mutation in the <i>GUSB</i> gene, the gene responsible for MPS VII. Enzyme replacement therapy was initiated, and the ascites was resolved. Careful systemic management, including lung-protective respiratory management and the early establishment of nutrition, is important for the long-term survival of infants with fetal hydrops, and early aggressive workup, including whole-genome sequencing for the cause, should be performed in the case of refractory ascites.</p>\",\"PeriodicalId\":7645,\"journal\":{\"name\":\"AJP Reports\",\"volume\":\"13 1\",\"pages\":\"e25-e28\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/da/a1/10-1055-a-2028-7784.PMC10019997.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AJP Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2028-7784\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AJP Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2028-7784","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
A Neonate with Mucopolysaccharidosis Type VII with Intractable Ascites.
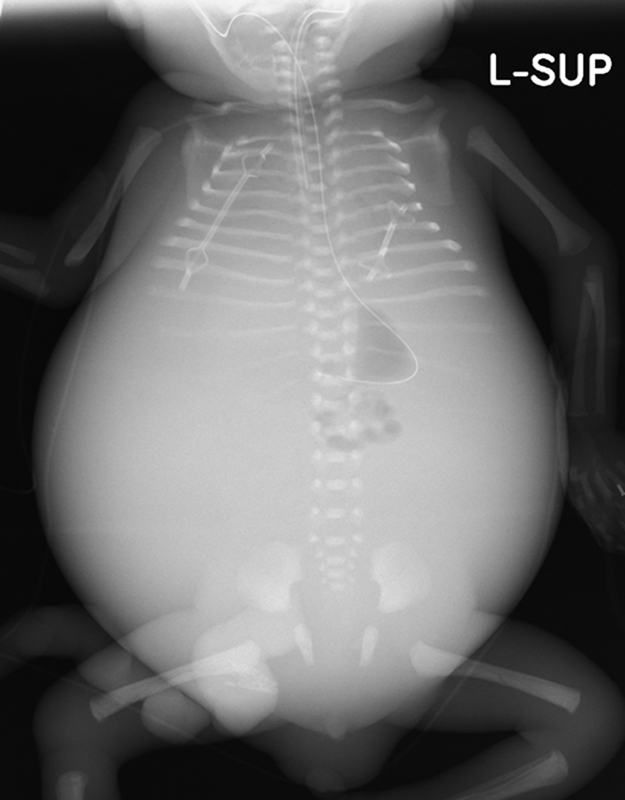
We report a case of a patient with severe fetal hydrops and refractory ascites, diagnosed as mucopolysaccharidosis type VII (MPS VII) by whole-exome sequencing, and discharged at 5 months of age after long-term ventilatory management. A male neonate was born by emergency cesarean section due to fetal distress at 30 1/7 weeks' gestation. Physical examination and X-rays revealed pleural effusion, ascites, and generalized edema, indicating severe fetal hydrops. He underwent tracheal intubation because of respiratory distress that was attributed to massive ascites, pulmonary hypoplasia, and pulmonary hypertension. He received mechanical ventilation and inhaled nitric oxide therapy. Prednisone, octreotide, and a factor XIII preparation were used as the treatment for ascites, and the ascites gradually decreased. He was extubated within 2 months of age. At 4 months of age, the results of whole-exome sequencing of the cord blood showed a compound heterozygous mutation in the GUSB gene, the gene responsible for MPS VII. Enzyme replacement therapy was initiated, and the ascites was resolved. Careful systemic management, including lung-protective respiratory management and the early establishment of nutrition, is important for the long-term survival of infants with fetal hydrops, and early aggressive workup, including whole-genome sequencing for the cause, should be performed in the case of refractory ascites.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


