{"title":"角膜胶原交联后中枢性中毒性角膜病变。","authors":"Mustafa Kayabasi, Canan A Utine","doi":"10.14744/bej.2023.38243","DOIUrl":null,"url":null,"abstract":"Dear Editor, Corneal collagen cross-linking (CXL) is a revolutionary procedure to halt keratoconus (KCN) progression, but it is not complication-free. Infectious keratitis, persistent epithelial defects, corneal edema, or severe melt have been reported after CXL (1). Most of the complications can be managed easily; some may lead to severe visual loss, such as central toxic keratopathy (CTK). Herein, we present six eyes of four patients that underwent CXL for progressive KCN elsewhere and, then, were referred to Dokuz Eylül University, Department of Ophthalmology with findings consistent with CTK (Table 1). Patients underwent detailed ophthalmological examination including corrected distance visual acuity (CDVA) on Snellen chart, slit-lamp examination, Scheimpflug corneal tomography (Pentacam, Oculus®, Germany), and specular microscopy (CellCheck, Konan®, United States). The study adhered to the tenets of Declaration of Helsinki. All patients complained of decreased vision after CXL with significant hyperopic shift. Slit-lamp examination revealed central corneal haze or scarring, vertical striae with indistinct margins, thinning and flattening, and clear peripheral cornea. No epithelial defect, epithelial laxity, staining patterns, stromal, or epithelial edema was detected. In Case 1, confocal microscopy showed acellular stroma, striations, and thick collagen bundles (Figs. 1a-c), and specular microscopy revealed endothelial cell count of 1602 cells/mm2 OD, 2181 cells/mm2 OS. In Case 2, significant inferior flattening at the tomography (Figs. 2a and b) was seen, whereas endothelial cell count was 2890 cells/mm2 OS on specular microscopy. Confocal or specular microscopy could not be performed in Cases 3 and 4; however, central corneal haze and associated significant flattening in the tomographies were evident (Figs. 3a and b, 4a and b). On consultation with their surgical-centers, patients’ operative histories were clarified. All cases had pre-operative thinnest de-epithelialized pachymetry of >400 μ and underwent accelerated de-epithelialized CXL protocol which included saturation of the stroma by instillation of 0.1% riboflavin solution (Riboflavin, Ricrolin, Peschke Meditrade, Germany) for a total 20 min and 365 nm ultraviolet-A (UVA) light application for 10 min at an irradiance of 9 mW/cm2, delivering a total dose of energy of 5.4 J/cm2. None of the cases developed infectious keratitis or diffuse lamellar keratitis (DLK) in the early postoperative period, and corneal healing was uneventful. Duration of the findings was at least 6 months in each case, with no resolution of the symptoms. Topical loteprednol bid, cyclosporine 0.05% bid, and carboxymethylcellulose qid treatments yielded no significant benefits in any of the cases. Topical cyclosporine 0.05% bid and peroral vitamin C 500 mg/day were commenced to provide anti-inflammatory effect and promote collagen re-synthesis and re-modeling in Mustafa Kayabasi, Canan A Utine","PeriodicalId":8740,"journal":{"name":"Beyoglu Eye Journal","volume":"8 1","pages":"69-72"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/b0/BEJ-8-69.PMC9993410.pdf","citationCount":"0","resultStr":"{\"title\":\"Central Toxic Keratopathy Following Corneal Collagen Cross-Linking.\",\"authors\":\"Mustafa Kayabasi, Canan A Utine\",\"doi\":\"10.14744/bej.2023.38243\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Dear Editor, Corneal collagen cross-linking (CXL) is a revolutionary procedure to halt keratoconus (KCN) progression, but it is not complication-free. Infectious keratitis, persistent epithelial defects, corneal edema, or severe melt have been reported after CXL (1). Most of the complications can be managed easily; some may lead to severe visual loss, such as central toxic keratopathy (CTK). Herein, we present six eyes of four patients that underwent CXL for progressive KCN elsewhere and, then, were referred to Dokuz Eylül University, Department of Ophthalmology with findings consistent with CTK (Table 1). Patients underwent detailed ophthalmological examination including corrected distance visual acuity (CDVA) on Snellen chart, slit-lamp examination, Scheimpflug corneal tomography (Pentacam, Oculus®, Germany), and specular microscopy (CellCheck, Konan®, United States). The study adhered to the tenets of Declaration of Helsinki. All patients complained of decreased vision after CXL with significant hyperopic shift. Slit-lamp examination revealed central corneal haze or scarring, vertical striae with indistinct margins, thinning and flattening, and clear peripheral cornea. No epithelial defect, epithelial laxity, staining patterns, stromal, or epithelial edema was detected. In Case 1, confocal microscopy showed acellular stroma, striations, and thick collagen bundles (Figs. 1a-c), and specular microscopy revealed endothelial cell count of 1602 cells/mm2 OD, 2181 cells/mm2 OS. In Case 2, significant inferior flattening at the tomography (Figs. 2a and b) was seen, whereas endothelial cell count was 2890 cells/mm2 OS on specular microscopy. Confocal or specular microscopy could not be performed in Cases 3 and 4; however, central corneal haze and associated significant flattening in the tomographies were evident (Figs. 3a and b, 4a and b). On consultation with their surgical-centers, patients’ operative histories were clarified. All cases had pre-operative thinnest de-epithelialized pachymetry of >400 μ and underwent accelerated de-epithelialized CXL protocol which included saturation of the stroma by instillation of 0.1% riboflavin solution (Riboflavin, Ricrolin, Peschke Meditrade, Germany) for a total 20 min and 365 nm ultraviolet-A (UVA) light application for 10 min at an irradiance of 9 mW/cm2, delivering a total dose of energy of 5.4 J/cm2. None of the cases developed infectious keratitis or diffuse lamellar keratitis (DLK) in the early postoperative period, and corneal healing was uneventful. Duration of the findings was at least 6 months in each case, with no resolution of the symptoms. Topical loteprednol bid, cyclosporine 0.05% bid, and carboxymethylcellulose qid treatments yielded no significant benefits in any of the cases. Topical cyclosporine 0.05% bid and peroral vitamin C 500 mg/day were commenced to provide anti-inflammatory effect and promote collagen re-synthesis and re-modeling in Mustafa Kayabasi, Canan A Utine\",\"PeriodicalId\":8740,\"journal\":{\"name\":\"Beyoglu Eye Journal\",\"volume\":\"8 1\",\"pages\":\"69-72\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/b0/BEJ-8-69.PMC9993410.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Beyoglu Eye Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14744/bej.2023.38243\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Beyoglu Eye Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/bej.2023.38243","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Central Toxic Keratopathy Following Corneal Collagen Cross-Linking.
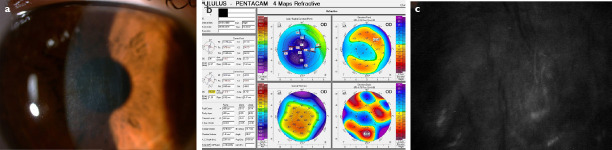
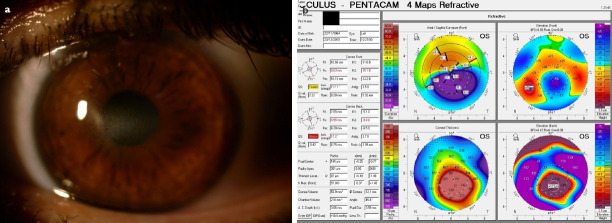
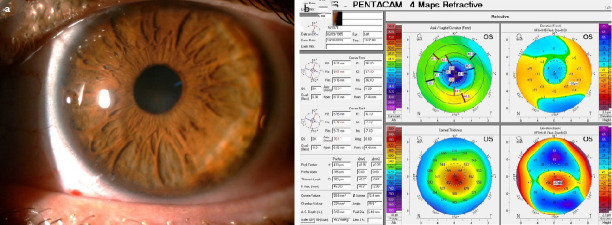
Dear Editor, Corneal collagen cross-linking (CXL) is a revolutionary procedure to halt keratoconus (KCN) progression, but it is not complication-free. Infectious keratitis, persistent epithelial defects, corneal edema, or severe melt have been reported after CXL (1). Most of the complications can be managed easily; some may lead to severe visual loss, such as central toxic keratopathy (CTK). Herein, we present six eyes of four patients that underwent CXL for progressive KCN elsewhere and, then, were referred to Dokuz Eylül University, Department of Ophthalmology with findings consistent with CTK (Table 1). Patients underwent detailed ophthalmological examination including corrected distance visual acuity (CDVA) on Snellen chart, slit-lamp examination, Scheimpflug corneal tomography (Pentacam, Oculus®, Germany), and specular microscopy (CellCheck, Konan®, United States). The study adhered to the tenets of Declaration of Helsinki. All patients complained of decreased vision after CXL with significant hyperopic shift. Slit-lamp examination revealed central corneal haze or scarring, vertical striae with indistinct margins, thinning and flattening, and clear peripheral cornea. No epithelial defect, epithelial laxity, staining patterns, stromal, or epithelial edema was detected. In Case 1, confocal microscopy showed acellular stroma, striations, and thick collagen bundles (Figs. 1a-c), and specular microscopy revealed endothelial cell count of 1602 cells/mm2 OD, 2181 cells/mm2 OS. In Case 2, significant inferior flattening at the tomography (Figs. 2a and b) was seen, whereas endothelial cell count was 2890 cells/mm2 OS on specular microscopy. Confocal or specular microscopy could not be performed in Cases 3 and 4; however, central corneal haze and associated significant flattening in the tomographies were evident (Figs. 3a and b, 4a and b). On consultation with their surgical-centers, patients’ operative histories were clarified. All cases had pre-operative thinnest de-epithelialized pachymetry of >400 μ and underwent accelerated de-epithelialized CXL protocol which included saturation of the stroma by instillation of 0.1% riboflavin solution (Riboflavin, Ricrolin, Peschke Meditrade, Germany) for a total 20 min and 365 nm ultraviolet-A (UVA) light application for 10 min at an irradiance of 9 mW/cm2, delivering a total dose of energy of 5.4 J/cm2. None of the cases developed infectious keratitis or diffuse lamellar keratitis (DLK) in the early postoperative period, and corneal healing was uneventful. Duration of the findings was at least 6 months in each case, with no resolution of the symptoms. Topical loteprednol bid, cyclosporine 0.05% bid, and carboxymethylcellulose qid treatments yielded no significant benefits in any of the cases. Topical cyclosporine 0.05% bid and peroral vitamin C 500 mg/day were commenced to provide anti-inflammatory effect and promote collagen re-synthesis and re-modeling in Mustafa Kayabasi, Canan A Utine

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


