{"title":"外侧入路保肌髋臼周围截骨术后外展肌恢复。","authors":"Yasuharu Nakashima, Daisuke Hara, Masanobu Ohishi, Goro Motomura, Ichiro Kawano, Satoshi Hamai, Shinya Kawahara, Taishi Sato, Ryosuke Yamaguchi, Takeshi Utsunomiya, Kenji Kitamura","doi":"10.1093/jhps/hnac047","DOIUrl":null,"url":null,"abstract":"<p><p>To decrease hip abductor dysfunction after periacetabular osteotomy using a lateral/trochanteric approach, we aimed to modify transposition osteotomy of the acetabulum (TOA) to not cut the greater trochanter and abductor-iliac crest detachment. We subsequently compared abductor muscle strength recovery between TOAs with [conventional TOA (C-TOA)] and without [modified TOA (M-TOA)] trochanteric osteotomy. C-TOA and M-TOA were performed in 27 and 34 hips, respectively. Hip abduction, flexion and knee extension muscle strength were measured preoperatively and at 3, 5, 10, 24 and 52 weeks postoperatively. The muscle strength ratio of the affected and contralateral lower limbs was compared between the C-TOA and M-TOA groups. Neither the mean Merle d'Aubigné-Postel score at the final follow-up nor the postoperative center-edge angle showed significant differences between the M-TOA and C-TOA groups (15.7 versus 16.4 points; <i>P</i> = 0.25 and 38.5° versus <i>P</i> = 0.62 and 39.8°, respectively). The mean muscle strength ratios of hip abduction at 5, 12 and 24 weeks postoperatively were significantly higher in the M-TOA group than in the C-TOA group (0.62 versus 0.39, 0.76 versus 0.59 and 0.94 versus 0.70; <i>P</i> = 0.03, 0.04 and 0.01, respectively). There were no significant differences between groups at Postoperative Week 52 (<i>P</i> = 0.36). Discomfort at the greater trochanter was observed in 18 hips (66.7%) in the C-TOA group but only in 4 hips (11.2%) in the M-TOA group. In conclusion, M-TOA is less invasive than C-TOA and allows an earlier recovery of abductor muscle strength without significant correction loss.</p>","PeriodicalId":48583,"journal":{"name":"Journal of Hip Preservation Surgery","volume":"9 4","pages":"259-264"},"PeriodicalIF":1.4000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/be/25/hnac047.PMC9993449.pdf","citationCount":"0","resultStr":"{\"title\":\"Abductor recovery after muscle-sparing periacetabular osteotomy using a lateral approach.\",\"authors\":\"Yasuharu Nakashima, Daisuke Hara, Masanobu Ohishi, Goro Motomura, Ichiro Kawano, Satoshi Hamai, Shinya Kawahara, Taishi Sato, Ryosuke Yamaguchi, Takeshi Utsunomiya, Kenji Kitamura\",\"doi\":\"10.1093/jhps/hnac047\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>To decrease hip abductor dysfunction after periacetabular osteotomy using a lateral/trochanteric approach, we aimed to modify transposition osteotomy of the acetabulum (TOA) to not cut the greater trochanter and abductor-iliac crest detachment. We subsequently compared abductor muscle strength recovery between TOAs with [conventional TOA (C-TOA)] and without [modified TOA (M-TOA)] trochanteric osteotomy. C-TOA and M-TOA were performed in 27 and 34 hips, respectively. Hip abduction, flexion and knee extension muscle strength were measured preoperatively and at 3, 5, 10, 24 and 52 weeks postoperatively. The muscle strength ratio of the affected and contralateral lower limbs was compared between the C-TOA and M-TOA groups. Neither the mean Merle d'Aubigné-Postel score at the final follow-up nor the postoperative center-edge angle showed significant differences between the M-TOA and C-TOA groups (15.7 versus 16.4 points; <i>P</i> = 0.25 and 38.5° versus <i>P</i> = 0.62 and 39.8°, respectively). The mean muscle strength ratios of hip abduction at 5, 12 and 24 weeks postoperatively were significantly higher in the M-TOA group than in the C-TOA group (0.62 versus 0.39, 0.76 versus 0.59 and 0.94 versus 0.70; <i>P</i> = 0.03, 0.04 and 0.01, respectively). There were no significant differences between groups at Postoperative Week 52 (<i>P</i> = 0.36). Discomfort at the greater trochanter was observed in 18 hips (66.7%) in the C-TOA group but only in 4 hips (11.2%) in the M-TOA group. In conclusion, M-TOA is less invasive than C-TOA and allows an earlier recovery of abductor muscle strength without significant correction loss.</p>\",\"PeriodicalId\":48583,\"journal\":{\"name\":\"Journal of Hip Preservation Surgery\",\"volume\":\"9 4\",\"pages\":\"259-264\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/be/25/hnac047.PMC9993449.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Hip Preservation Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/jhps/hnac047\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hip Preservation Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/jhps/hnac047","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
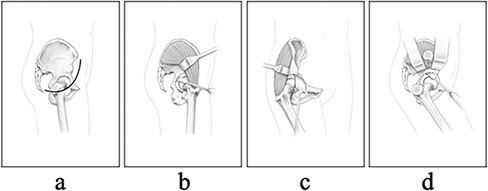
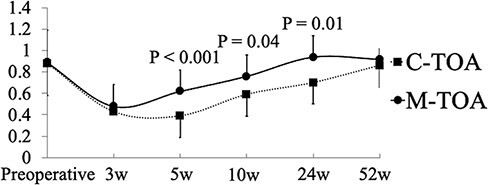
为了减少髋臼周围行外侧/粗隆入路截骨后髋外展肌功能障碍,我们的目的是修改髋臼转位截骨术(TOA),使其不切割大转子和外展髂骨脱离。随后,我们比较了[常规TOA (C-TOA)]和[改良TOA (M-TOA)]转子截骨术的外展肌力量恢复情况。C-TOA和M-TOA分别在27髋和34髋进行。术前及术后3周、5周、10周、24周和52周分别测量髋关节外展、屈曲和膝关节伸肌力量。比较C-TOA组和M-TOA组患侧和对侧下肢肌力比。M-TOA组和C-TOA组在最后随访时Merle d' aubigne - postel平均评分和术后中心边缘角均无显著差异(15.7分对16.4分;P = 0.25和38.5°,P = 0.62和39.8°)。术后5周、12周和24周,M-TOA组髋外展的平均肌力比明显高于C-TOA组(0.62 vs 0.39, 0.76 vs 0.59, 0.94 vs 0.70;P分别= 0.03、0.04、0.01)。术后第52周各组间差异无统计学意义(P = 0.36)。C-TOA组有18髋(66.7%)出现大转子不适,而M-TOA组只有4髋(11.2%)。综上所述,M-TOA比C-TOA侵入性更小,可以更早地恢复外展肌力量,而不会造成明显的矫正损失。
Abductor recovery after muscle-sparing periacetabular osteotomy using a lateral approach.
To decrease hip abductor dysfunction after periacetabular osteotomy using a lateral/trochanteric approach, we aimed to modify transposition osteotomy of the acetabulum (TOA) to not cut the greater trochanter and abductor-iliac crest detachment. We subsequently compared abductor muscle strength recovery between TOAs with [conventional TOA (C-TOA)] and without [modified TOA (M-TOA)] trochanteric osteotomy. C-TOA and M-TOA were performed in 27 and 34 hips, respectively. Hip abduction, flexion and knee extension muscle strength were measured preoperatively and at 3, 5, 10, 24 and 52 weeks postoperatively. The muscle strength ratio of the affected and contralateral lower limbs was compared between the C-TOA and M-TOA groups. Neither the mean Merle d'Aubigné-Postel score at the final follow-up nor the postoperative center-edge angle showed significant differences between the M-TOA and C-TOA groups (15.7 versus 16.4 points; P = 0.25 and 38.5° versus P = 0.62 and 39.8°, respectively). The mean muscle strength ratios of hip abduction at 5, 12 and 24 weeks postoperatively were significantly higher in the M-TOA group than in the C-TOA group (0.62 versus 0.39, 0.76 versus 0.59 and 0.94 versus 0.70; P = 0.03, 0.04 and 0.01, respectively). There were no significant differences between groups at Postoperative Week 52 (P = 0.36). Discomfort at the greater trochanter was observed in 18 hips (66.7%) in the C-TOA group but only in 4 hips (11.2%) in the M-TOA group. In conclusion, M-TOA is less invasive than C-TOA and allows an earlier recovery of abductor muscle strength without significant correction loss.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


