Benedikt Marahrens, Leah Damsch, Rebecca Lehmann, Igor Matyukhin, Susann Patschan, Daniel Patschan
{"title":"急性肾损伤发病时血清钠升高预测院内死亡","authors":"Benedikt Marahrens, Leah Damsch, Rebecca Lehmann, Igor Matyukhin, Susann Patschan, Daniel Patschan","doi":"10.14740/jocmr4845","DOIUrl":null,"url":null,"abstract":"Background Over the last decades, acute kidney injury (AKI) has been identified as a potentially fatal diagnosis which substantially increases in-hospital mortality in the short term and morbidity/mortality in the long term. However, reliable biomarkers for predicting AKI-associated outcomes are still missing. In this study, we assessed whether serum sodium, measured at different time points during the in-hospital treatment period, provided prognostic information in AKI. Methods This was a retrospective, observational cohort study. AKI subjects were identified via the in-hospital AKI alert system. Serum sodium and potassium levels were documented at five pre-defined time points: hospital admission, AKI onset, minimum estimated glomerular filtration rate, minimum and maximum of the respective electrolyte during the treatment period. In-hospital death, the need for kidney replacement therapy (KRT) and recovery of kidney function were defined as endpoints. Results Patients who suffered in-hospital death (n = 37, 23.1%) showed significantly higher serum sodium levels at diagnosis of AKI (survivors: 145.7 ± 2.13 vs. non-survivors: 138.8 ± 0.636 mmol/L, P = 0.003). A logistic regression model was significant for serum sodium levels in patients with in-hospital death (X2, P = 0.003; odds ratio = 1.08 (1.022 - 1.141); R2 = 0.082; d = 0.089). This suggests an increase of the relative risk for in-hospital death by 8% with every unit of serum sodium increase. Patients with a sodium above the upper normal range at AKI diagnosis were also more likely to suffer in-hospital death (P = 0.001). Conclusion In summary, we present evidence that serum sodium, measured at time of AKI diagnosis, potentially serves as a predictor for in-hospital death in patients with AKI.","PeriodicalId":15431,"journal":{"name":"Journal of Clinical Medicine Research","volume":"15 2","pages":"90-98"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e5/91/jocmr-15-090.PMC9990719.pdf","citationCount":"1","resultStr":"{\"title\":\"Increased Serum Sodium at Acute Kidney Injury Onset Predicts In-Hospital Death.\",\"authors\":\"Benedikt Marahrens, Leah Damsch, Rebecca Lehmann, Igor Matyukhin, Susann Patschan, Daniel Patschan\",\"doi\":\"10.14740/jocmr4845\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Background Over the last decades, acute kidney injury (AKI) has been identified as a potentially fatal diagnosis which substantially increases in-hospital mortality in the short term and morbidity/mortality in the long term. However, reliable biomarkers for predicting AKI-associated outcomes are still missing. In this study, we assessed whether serum sodium, measured at different time points during the in-hospital treatment period, provided prognostic information in AKI. Methods This was a retrospective, observational cohort study. AKI subjects were identified via the in-hospital AKI alert system. Serum sodium and potassium levels were documented at five pre-defined time points: hospital admission, AKI onset, minimum estimated glomerular filtration rate, minimum and maximum of the respective electrolyte during the treatment period. In-hospital death, the need for kidney replacement therapy (KRT) and recovery of kidney function were defined as endpoints. Results Patients who suffered in-hospital death (n = 37, 23.1%) showed significantly higher serum sodium levels at diagnosis of AKI (survivors: 145.7 ± 2.13 vs. non-survivors: 138.8 ± 0.636 mmol/L, P = 0.003). A logistic regression model was significant for serum sodium levels in patients with in-hospital death (X2, P = 0.003; odds ratio = 1.08 (1.022 - 1.141); R2 = 0.082; d = 0.089). This suggests an increase of the relative risk for in-hospital death by 8% with every unit of serum sodium increase. Patients with a sodium above the upper normal range at AKI diagnosis were also more likely to suffer in-hospital death (P = 0.001). Conclusion In summary, we present evidence that serum sodium, measured at time of AKI diagnosis, potentially serves as a predictor for in-hospital death in patients with AKI.\",\"PeriodicalId\":15431,\"journal\":{\"name\":\"Journal of Clinical Medicine Research\",\"volume\":\"15 2\",\"pages\":\"90-98\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e5/91/jocmr-15-090.PMC9990719.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Medicine Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jocmr4845\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr4845","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
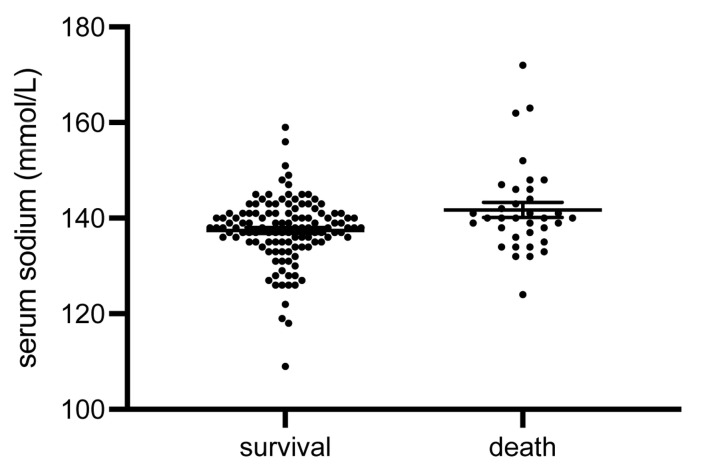
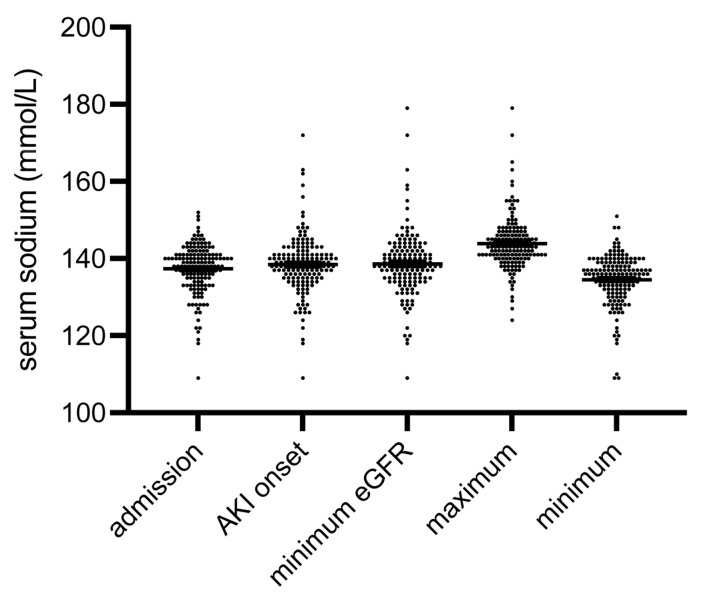
Background Over the last decades, acute kidney injury (AKI) has been identified as a potentially fatal diagnosis which substantially increases in-hospital mortality in the short term and morbidity/mortality in the long term. However, reliable biomarkers for predicting AKI-associated outcomes are still missing. In this study, we assessed whether serum sodium, measured at different time points during the in-hospital treatment period, provided prognostic information in AKI. Methods This was a retrospective, observational cohort study. AKI subjects were identified via the in-hospital AKI alert system. Serum sodium and potassium levels were documented at five pre-defined time points: hospital admission, AKI onset, minimum estimated glomerular filtration rate, minimum and maximum of the respective electrolyte during the treatment period. In-hospital death, the need for kidney replacement therapy (KRT) and recovery of kidney function were defined as endpoints. Results Patients who suffered in-hospital death (n = 37, 23.1%) showed significantly higher serum sodium levels at diagnosis of AKI (survivors: 145.7 ± 2.13 vs. non-survivors: 138.8 ± 0.636 mmol/L, P = 0.003). A logistic regression model was significant for serum sodium levels in patients with in-hospital death (X2, P = 0.003; odds ratio = 1.08 (1.022 - 1.141); R2 = 0.082; d = 0.089). This suggests an increase of the relative risk for in-hospital death by 8% with every unit of serum sodium increase. Patients with a sodium above the upper normal range at AKI diagnosis were also more likely to suffer in-hospital death (P = 0.001). Conclusion In summary, we present evidence that serum sodium, measured at time of AKI diagnosis, potentially serves as a predictor for in-hospital death in patients with AKI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


