Maryum Merchant, Scott B Hu, Stella Cohen, Peter H Grossman, Kurt M Richards, Malcolm I Smith
{"title":"对重大烧伤患者减少定向输液后的效果进行评估。","authors":"Maryum Merchant, Scott B Hu, Stella Cohen, Peter H Grossman, Kurt M Richards, Malcolm I Smith","doi":"10.3390/ebj4020021","DOIUrl":null,"url":null,"abstract":"<p><p>Adequate fluid resuscitation in adults with major burns is crucial to prevent or minimize burn shock, but needs to be balanced against the complications of over-resuscitation. A single-center, retrospective review of 95 ICU patients with severe burns from Jan 2014 to Aug 2021 was performed. Some 52 patients were managed with a liberal targeted fluid goal of 4 mL/kg/%TBSA, and 43 patients were managed after we incorporated a restricted fluid goal of 2 mL/kg/%TBSA into our standard resuscitation strategy. Of the 95 patients included in this analysis, 76 patients (80%) survived admission. The median age was 41 years, and the median TBSA was 36%. All patients received Ringer's lactate as the primary fluid for resuscitation, and 40 of the 95 patients (42%) received colloids as a rescue infusion within 24 h of injury. Some 44 of the 95 patients (46.3%) had a concurrent inhalational injury. The median length of hospital stay was 37 days, and the median ICU length of stay was 18 days. A total of 17 of the 95 patients developed ARDS (17.9%), 51 of the 95 (53.7%) patients developed pneumonia, and 34 of the 95 patients (35.8%) developed AKI within the first 7 days of admission. The median fluid administered during the first day of hospitalization from 2019 onwards remained close to 4 mL/kg/%TBSA, despite transitioning to a 2 mL/kg/%TBSA formula for a 24 h fluid goal (unless there was an electrical burn, in which case the 4 cc/kg formula was utilized). Further exploratory analyses also suggested that under-resuscitation and administration of albumin may be associated with increased mortality, though this did not reach statistical significance. ARDS development was associated with increased age and TBSA as well as increased fluid intake within the first 24 h. A change in the targeted fluid goal from liberal (4 mL/kg/%TBSA) to a restricted (2 mL/kg/%TBSA) formula did not change the actual fluids administered over 24 h when guided by clinical criteria. Our review did suggest that under-resuscitation contributed to mortality, but that excessive fluid resuscitation likely contributed to ARDS risks for large TBSA patients. Our data suggest that strategies to optimize fluid administration are important to improve patient outcomes, but should focus on clinical parameters rather than calculated fluid goals.</p>","PeriodicalId":72961,"journal":{"name":"European burn journal","volume":"1 1","pages":"234-247"},"PeriodicalIF":1.2000,"publicationDate":"2023-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11571837/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of Outcomes following Reduction in Targeted Fluid Administration in Major Burns.\",\"authors\":\"Maryum Merchant, Scott B Hu, Stella Cohen, Peter H Grossman, Kurt M Richards, Malcolm I Smith\",\"doi\":\"10.3390/ebj4020021\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Adequate fluid resuscitation in adults with major burns is crucial to prevent or minimize burn shock, but needs to be balanced against the complications of over-resuscitation. A single-center, retrospective review of 95 ICU patients with severe burns from Jan 2014 to Aug 2021 was performed. Some 52 patients were managed with a liberal targeted fluid goal of 4 mL/kg/%TBSA, and 43 patients were managed after we incorporated a restricted fluid goal of 2 mL/kg/%TBSA into our standard resuscitation strategy. Of the 95 patients included in this analysis, 76 patients (80%) survived admission. The median age was 41 years, and the median TBSA was 36%. All patients received Ringer's lactate as the primary fluid for resuscitation, and 40 of the 95 patients (42%) received colloids as a rescue infusion within 24 h of injury. Some 44 of the 95 patients (46.3%) had a concurrent inhalational injury. The median length of hospital stay was 37 days, and the median ICU length of stay was 18 days. A total of 17 of the 95 patients developed ARDS (17.9%), 51 of the 95 (53.7%) patients developed pneumonia, and 34 of the 95 patients (35.8%) developed AKI within the first 7 days of admission. The median fluid administered during the first day of hospitalization from 2019 onwards remained close to 4 mL/kg/%TBSA, despite transitioning to a 2 mL/kg/%TBSA formula for a 24 h fluid goal (unless there was an electrical burn, in which case the 4 cc/kg formula was utilized). Further exploratory analyses also suggested that under-resuscitation and administration of albumin may be associated with increased mortality, though this did not reach statistical significance. ARDS development was associated with increased age and TBSA as well as increased fluid intake within the first 24 h. A change in the targeted fluid goal from liberal (4 mL/kg/%TBSA) to a restricted (2 mL/kg/%TBSA) formula did not change the actual fluids administered over 24 h when guided by clinical criteria. Our review did suggest that under-resuscitation contributed to mortality, but that excessive fluid resuscitation likely contributed to ARDS risks for large TBSA patients. Our data suggest that strategies to optimize fluid administration are important to improve patient outcomes, but should focus on clinical parameters rather than calculated fluid goals.</p>\",\"PeriodicalId\":72961,\"journal\":{\"name\":\"European burn journal\",\"volume\":\"1 1\",\"pages\":\"234-247\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11571837/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European burn journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/ebj4020021\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European burn journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/ebj4020021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Evaluation of Outcomes following Reduction in Targeted Fluid Administration in Major Burns.
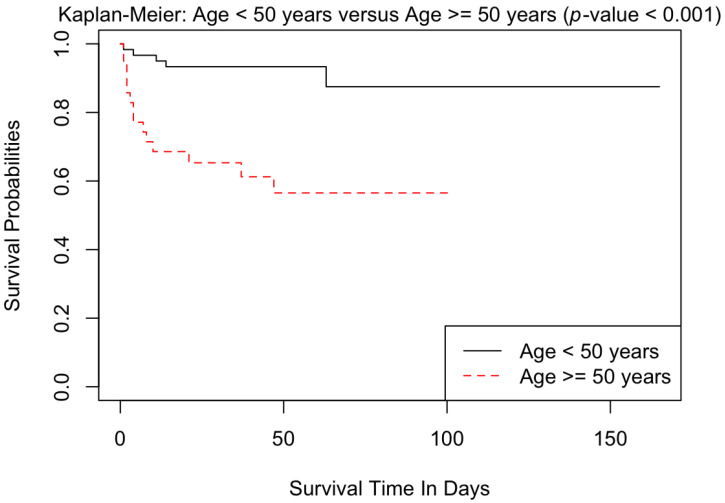
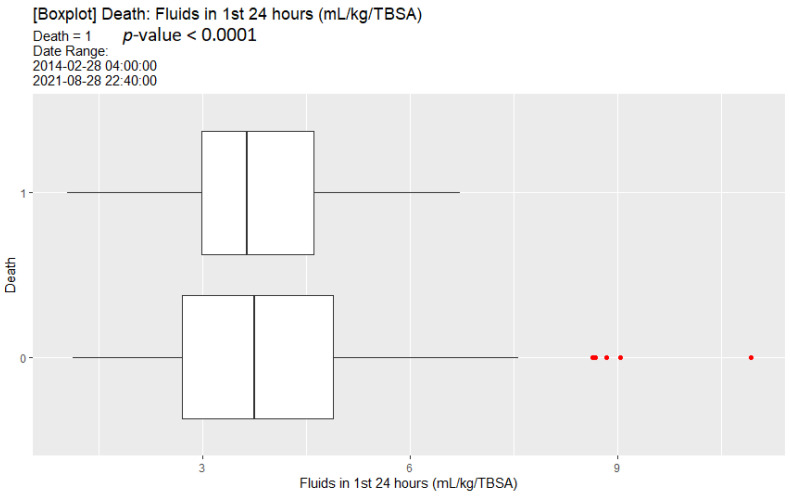
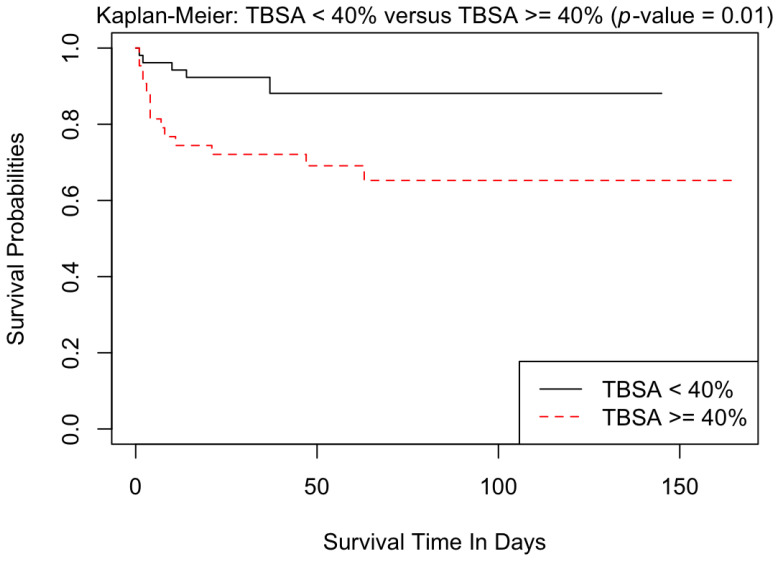
Adequate fluid resuscitation in adults with major burns is crucial to prevent or minimize burn shock, but needs to be balanced against the complications of over-resuscitation. A single-center, retrospective review of 95 ICU patients with severe burns from Jan 2014 to Aug 2021 was performed. Some 52 patients were managed with a liberal targeted fluid goal of 4 mL/kg/%TBSA, and 43 patients were managed after we incorporated a restricted fluid goal of 2 mL/kg/%TBSA into our standard resuscitation strategy. Of the 95 patients included in this analysis, 76 patients (80%) survived admission. The median age was 41 years, and the median TBSA was 36%. All patients received Ringer's lactate as the primary fluid for resuscitation, and 40 of the 95 patients (42%) received colloids as a rescue infusion within 24 h of injury. Some 44 of the 95 patients (46.3%) had a concurrent inhalational injury. The median length of hospital stay was 37 days, and the median ICU length of stay was 18 days. A total of 17 of the 95 patients developed ARDS (17.9%), 51 of the 95 (53.7%) patients developed pneumonia, and 34 of the 95 patients (35.8%) developed AKI within the first 7 days of admission. The median fluid administered during the first day of hospitalization from 2019 onwards remained close to 4 mL/kg/%TBSA, despite transitioning to a 2 mL/kg/%TBSA formula for a 24 h fluid goal (unless there was an electrical burn, in which case the 4 cc/kg formula was utilized). Further exploratory analyses also suggested that under-resuscitation and administration of albumin may be associated with increased mortality, though this did not reach statistical significance. ARDS development was associated with increased age and TBSA as well as increased fluid intake within the first 24 h. A change in the targeted fluid goal from liberal (4 mL/kg/%TBSA) to a restricted (2 mL/kg/%TBSA) formula did not change the actual fluids administered over 24 h when guided by clinical criteria. Our review did suggest that under-resuscitation contributed to mortality, but that excessive fluid resuscitation likely contributed to ARDS risks for large TBSA patients. Our data suggest that strategies to optimize fluid administration are important to improve patient outcomes, but should focus on clinical parameters rather than calculated fluid goals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


