{"title":"射血分数降低型心力衰竭(HFrEF)患者功能性二尖瓣反流严重程度的临床意义。","authors":"Nabil Naser","doi":"10.5455/medarh.2022.76.17-22","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>An estimated 64.3 million people are living with heart failure worldwide. Functional MR in chronic HFrEF reflects primarily the severity of LV dysfunction and is not related to structural alterations of the mitral valvular apparatus. FMR in patients with HFrEF independently of the etiology of HFrEF and its underlying mechanisms, contributes to progression of the symptoms of HF and is independent predictor of worse clinical outcomes.</p><p><strong>Objective: </strong>The purpose of this study was to assess the severity of functional mitral regurgitation (FMR) and its clinical implications in patients with chronic heart failure with reduced ejection fraction (HFrEF).</p><p><strong>Methods: </strong>We enrolled 146 consecutive adult patients with CHF with reduced ejection fraction (HFrEF) who presented to outpatient clinics. All patients underwent clinical and physical examination. Baseline examination included medical history, detailed assessment of current medication, electrocardiogram recording, transthoracic echocardiogram and comorbidities. Heart failure with reduced ejection fraction was defined in line with the new guidelines as history of HF signs and symptoms as well as a LV ejection fraction (LVEF) below 40%. Cardiovascular risk factors were recorded according to the respective guidelines. FMR was defined and graded according to the ESC/EACTS Guidelines for the management of valvular heart disease. The extent of FMR was assessed at baseline and after a median follow-up period of 4 years in 146 consecutive HFrEF patients (left ventricular ejection fraction <40%). All of the patients received the heart failure (HF) medications in agreement with 2016 and 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Major adverse cardiac events were defined as a composite of all-cause death and the need for admission for HF.</p><p><strong>Results: </strong>A total of 146 chronic HFrEF patients (mean age of 63±11 years, 62% male, mean LVEF of 25±11%) of which 19% patients had severe FMR at baseline, with a mean EROA of 31.4±2.7 mm2 and a mean Reg Vol of 45.9±5.3 ml. There was a significant interaction between FMR and NYHA functional class in predicting death or need for hospitalization, (P < 0.0001 for the interaction term FMR NYHA III-IV). During a median follow-up period of 4.2 (IQR) 3.1-5.8) years, the primary endpoint occurred in 52 (36%) patients (21 HF admissions, and 31 deaths). There was a strong graded association between the presence and degree of FMR and risk of death or admission (P <0.0001) at 4 years follow-up period. Regarding HF therapy, 129 patients (88%) received RAAS antagonists, 17 patients (12%) received ARNI, 86 patients (59%) received beta-blockers, 75 patients (51%) were treated with MRA. 31 patients (21%) underwent cardiac resynchronization therapy (CRT) with a response rate of 64%. 24 patients (16%) underwent ICD implantation.</p><p><strong>Conclusion: </strong>Guideline-directed medical therapy is the first-line treatment for chronic HF patients who also have FMR. After this first-line approach, surgical or MitraClip transcatheter therapy can be considered in patients with persistent severe and symptomatic FMR in order to improve symptoms, quality of life and functional status.</p>","PeriodicalId":13309,"journal":{"name":"Implant Dentistry","volume":"26 1","pages":"17-22"},"PeriodicalIF":0.0000,"publicationDate":"2022-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8976892/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Implications of Functional Mitral Regurgitation Severity in Patients with Heart Failure with Reduced Ejection Fraction (HFrEF).\",\"authors\":\"Nabil Naser\",\"doi\":\"10.5455/medarh.2022.76.17-22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>An estimated 64.3 million people are living with heart failure worldwide. Functional MR in chronic HFrEF reflects primarily the severity of LV dysfunction and is not related to structural alterations of the mitral valvular apparatus. FMR in patients with HFrEF independently of the etiology of HFrEF and its underlying mechanisms, contributes to progression of the symptoms of HF and is independent predictor of worse clinical outcomes.</p><p><strong>Objective: </strong>The purpose of this study was to assess the severity of functional mitral regurgitation (FMR) and its clinical implications in patients with chronic heart failure with reduced ejection fraction (HFrEF).</p><p><strong>Methods: </strong>We enrolled 146 consecutive adult patients with CHF with reduced ejection fraction (HFrEF) who presented to outpatient clinics. All patients underwent clinical and physical examination. Baseline examination included medical history, detailed assessment of current medication, electrocardiogram recording, transthoracic echocardiogram and comorbidities. Heart failure with reduced ejection fraction was defined in line with the new guidelines as history of HF signs and symptoms as well as a LV ejection fraction (LVEF) below 40%. Cardiovascular risk factors were recorded according to the respective guidelines. FMR was defined and graded according to the ESC/EACTS Guidelines for the management of valvular heart disease. The extent of FMR was assessed at baseline and after a median follow-up period of 4 years in 146 consecutive HFrEF patients (left ventricular ejection fraction <40%). All of the patients received the heart failure (HF) medications in agreement with 2016 and 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Major adverse cardiac events were defined as a composite of all-cause death and the need for admission for HF.</p><p><strong>Results: </strong>A total of 146 chronic HFrEF patients (mean age of 63±11 years, 62% male, mean LVEF of 25±11%) of which 19% patients had severe FMR at baseline, with a mean EROA of 31.4±2.7 mm2 and a mean Reg Vol of 45.9±5.3 ml. There was a significant interaction between FMR and NYHA functional class in predicting death or need for hospitalization, (P < 0.0001 for the interaction term FMR NYHA III-IV). During a median follow-up period of 4.2 (IQR) 3.1-5.8) years, the primary endpoint occurred in 52 (36%) patients (21 HF admissions, and 31 deaths). There was a strong graded association between the presence and degree of FMR and risk of death or admission (P <0.0001) at 4 years follow-up period. Regarding HF therapy, 129 patients (88%) received RAAS antagonists, 17 patients (12%) received ARNI, 86 patients (59%) received beta-blockers, 75 patients (51%) were treated with MRA. 31 patients (21%) underwent cardiac resynchronization therapy (CRT) with a response rate of 64%. 24 patients (16%) underwent ICD implantation.</p><p><strong>Conclusion: </strong>Guideline-directed medical therapy is the first-line treatment for chronic HF patients who also have FMR. After this first-line approach, surgical or MitraClip transcatheter therapy can be considered in patients with persistent severe and symptomatic FMR in order to improve symptoms, quality of life and functional status.</p>\",\"PeriodicalId\":13309,\"journal\":{\"name\":\"Implant Dentistry\",\"volume\":\"26 1\",\"pages\":\"17-22\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8976892/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Implant Dentistry\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5455/medarh.2022.76.17-22\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Dentistry\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implant Dentistry","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5455/medarh.2022.76.17-22","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Dentistry","Score":null,"Total":0}
Clinical Implications of Functional Mitral Regurgitation Severity in Patients with Heart Failure with Reduced Ejection Fraction (HFrEF).
Background: An estimated 64.3 million people are living with heart failure worldwide. Functional MR in chronic HFrEF reflects primarily the severity of LV dysfunction and is not related to structural alterations of the mitral valvular apparatus. FMR in patients with HFrEF independently of the etiology of HFrEF and its underlying mechanisms, contributes to progression of the symptoms of HF and is independent predictor of worse clinical outcomes.
Objective: The purpose of this study was to assess the severity of functional mitral regurgitation (FMR) and its clinical implications in patients with chronic heart failure with reduced ejection fraction (HFrEF).
Methods: We enrolled 146 consecutive adult patients with CHF with reduced ejection fraction (HFrEF) who presented to outpatient clinics. All patients underwent clinical and physical examination. Baseline examination included medical history, detailed assessment of current medication, electrocardiogram recording, transthoracic echocardiogram and comorbidities. Heart failure with reduced ejection fraction was defined in line with the new guidelines as history of HF signs and symptoms as well as a LV ejection fraction (LVEF) below 40%. Cardiovascular risk factors were recorded according to the respective guidelines. FMR was defined and graded according to the ESC/EACTS Guidelines for the management of valvular heart disease. The extent of FMR was assessed at baseline and after a median follow-up period of 4 years in 146 consecutive HFrEF patients (left ventricular ejection fraction <40%). All of the patients received the heart failure (HF) medications in agreement with 2016 and 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Major adverse cardiac events were defined as a composite of all-cause death and the need for admission for HF.
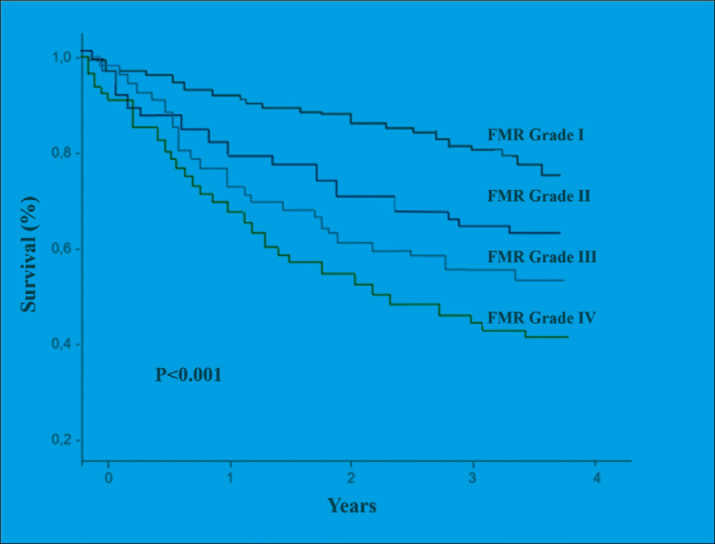
Results: A total of 146 chronic HFrEF patients (mean age of 63±11 years, 62% male, mean LVEF of 25±11%) of which 19% patients had severe FMR at baseline, with a mean EROA of 31.4±2.7 mm2 and a mean Reg Vol of 45.9±5.3 ml. There was a significant interaction between FMR and NYHA functional class in predicting death or need for hospitalization, (P < 0.0001 for the interaction term FMR NYHA III-IV). During a median follow-up period of 4.2 (IQR) 3.1-5.8) years, the primary endpoint occurred in 52 (36%) patients (21 HF admissions, and 31 deaths). There was a strong graded association between the presence and degree of FMR and risk of death or admission (P <0.0001) at 4 years follow-up period. Regarding HF therapy, 129 patients (88%) received RAAS antagonists, 17 patients (12%) received ARNI, 86 patients (59%) received beta-blockers, 75 patients (51%) were treated with MRA. 31 patients (21%) underwent cardiac resynchronization therapy (CRT) with a response rate of 64%. 24 patients (16%) underwent ICD implantation.
Conclusion: Guideline-directed medical therapy is the first-line treatment for chronic HF patients who also have FMR. After this first-line approach, surgical or MitraClip transcatheter therapy can be considered in patients with persistent severe and symptomatic FMR in order to improve symptoms, quality of life and functional status.
期刊介绍:
Cessation. Implant Dentistry, an interdisciplinary forum for general practitioners, specialists, educators, and researchers, publishes relevant clinical, educational, and research articles that document current concepts of oral implantology in sections on biomaterials, clinical reports, oral and maxillofacial surgery, oral pathology, periodontics, prosthodontics, and research. The journal includes guest editorials, letters to the editor, book reviews, abstracts of current literature, and news of sponsoring societies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


