Xinfang Lv, Xue Wu, Kai Liu, Xinke Zhao, Chenliang Pan, Jing Zhao, Juan Chang, Huan Guo, Xiang Gao, Xiaodong Zhi, Chunzhen Ren, Qilin Chen, Hugang Jiang, Chunling Wang, Ying-Dong Li
{"title":"预测食管癌症放疗后心脏死亡的列线图的开发和验证","authors":"Xinfang Lv, Xue Wu, Kai Liu, Xinke Zhao, Chenliang Pan, Jing Zhao, Juan Chang, Huan Guo, Xiang Gao, Xiaodong Zhi, Chunzhen Ren, Qilin Chen, Hugang Jiang, Chunling Wang, Ying-Dong Li","doi":"10.1002/cai2.89","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Patients frequently die from cardiac causes after radiotherapy for esophageal cancer. Early detection of cardiac death risk in these patients is crucial to improve clinical decision-making and prognosis. Thus, we modeled the risk of cardiac death after irradiation for esophageal cancer.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A retrospective analysis of 37,599 esophageal cancer cases treated with radiotherapy in the SEER database between 2000 and 2018 was performed. The selected cases were randomly assigned to the model development group (<i>n</i> = 26,320) and model validation group (<i>n</i> = 11,279) at a ratio of 7:3. We identified the risk factors most commonly associated with cardiac death by least absolute shrinkage and selection operator regression analysis (LASSO). The endpoints for model development and validation were 5- and 10-year survival rates. The net clinical benefit of the models was evaluated by decision curve analysis (DCA) and concordance index (C-index). The performance of the models was further assessed by creating a receiver operating characteristic curve (ROC) and calculating the area under the curve (AUC). Kaplan-Meier (K-M) survival analysis was performed on the probability of death. Patients were classified according to death probability thresholds. Five- and ten-year survival rates for the two groups were shown using K-M curves.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The major risk factors for cardiac death were age, surgery, year of diagnosis, sequence of surgery and radiotherapy, chemotherapy and a number of tumors, which were used to create the nomogram. The C-indexes of the nomograms were 0.708 and 0.679 for the development and validation groups, respectively. DCA showed the good net clinical benefit of nomograms in predicting 5- and 10-year risk of cardiac death. The model exhibited moderate predictive power for 5- and 10-year cardiac mortality (AUC: 0.833 and 0.854, respectively), and for the development and validation cohorts (AUC: 0.76 and 0.813, respectively).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Our nomogram may assist clinicians in making clinical decisions about patients undergoing radiotherapy for esophageal cancer based on early detection of cardiac death risk.</p>\n </section>\n </div>","PeriodicalId":100212,"journal":{"name":"Cancer Innovation","volume":"2 5","pages":"391-404"},"PeriodicalIF":2.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Development and validation of a nomogram to predict cardiac death after radiotherapy for esophageal cancer\",\"authors\":\"Xinfang Lv, Xue Wu, Kai Liu, Xinke Zhao, Chenliang Pan, Jing Zhao, Juan Chang, Huan Guo, Xiang Gao, Xiaodong Zhi, Chunzhen Ren, Qilin Chen, Hugang Jiang, Chunling Wang, Ying-Dong Li\",\"doi\":\"10.1002/cai2.89\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Patients frequently die from cardiac causes after radiotherapy for esophageal cancer. Early detection of cardiac death risk in these patients is crucial to improve clinical decision-making and prognosis. Thus, we modeled the risk of cardiac death after irradiation for esophageal cancer.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A retrospective analysis of 37,599 esophageal cancer cases treated with radiotherapy in the SEER database between 2000 and 2018 was performed. The selected cases were randomly assigned to the model development group (<i>n</i> = 26,320) and model validation group (<i>n</i> = 11,279) at a ratio of 7:3. We identified the risk factors most commonly associated with cardiac death by least absolute shrinkage and selection operator regression analysis (LASSO). The endpoints for model development and validation were 5- and 10-year survival rates. The net clinical benefit of the models was evaluated by decision curve analysis (DCA) and concordance index (C-index). The performance of the models was further assessed by creating a receiver operating characteristic curve (ROC) and calculating the area under the curve (AUC). Kaplan-Meier (K-M) survival analysis was performed on the probability of death. Patients were classified according to death probability thresholds. Five- and ten-year survival rates for the two groups were shown using K-M curves.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The major risk factors for cardiac death were age, surgery, year of diagnosis, sequence of surgery and radiotherapy, chemotherapy and a number of tumors, which were used to create the nomogram. The C-indexes of the nomograms were 0.708 and 0.679 for the development and validation groups, respectively. DCA showed the good net clinical benefit of nomograms in predicting 5- and 10-year risk of cardiac death. The model exhibited moderate predictive power for 5- and 10-year cardiac mortality (AUC: 0.833 and 0.854, respectively), and for the development and validation cohorts (AUC: 0.76 and 0.813, respectively).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Our nomogram may assist clinicians in making clinical decisions about patients undergoing radiotherapy for esophageal cancer based on early detection of cardiac death risk.</p>\\n </section>\\n </div>\",\"PeriodicalId\":100212,\"journal\":{\"name\":\"Cancer Innovation\",\"volume\":\"2 5\",\"pages\":\"391-404\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Innovation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cai2.89\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Innovation","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cai2.89","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Development and validation of a nomogram to predict cardiac death after radiotherapy for esophageal cancer
Background
Patients frequently die from cardiac causes after radiotherapy for esophageal cancer. Early detection of cardiac death risk in these patients is crucial to improve clinical decision-making and prognosis. Thus, we modeled the risk of cardiac death after irradiation for esophageal cancer.
Methods
A retrospective analysis of 37,599 esophageal cancer cases treated with radiotherapy in the SEER database between 2000 and 2018 was performed. The selected cases were randomly assigned to the model development group (n = 26,320) and model validation group (n = 11,279) at a ratio of 7:3. We identified the risk factors most commonly associated with cardiac death by least absolute shrinkage and selection operator regression analysis (LASSO). The endpoints for model development and validation were 5- and 10-year survival rates. The net clinical benefit of the models was evaluated by decision curve analysis (DCA) and concordance index (C-index). The performance of the models was further assessed by creating a receiver operating characteristic curve (ROC) and calculating the area under the curve (AUC). Kaplan-Meier (K-M) survival analysis was performed on the probability of death. Patients were classified according to death probability thresholds. Five- and ten-year survival rates for the two groups were shown using K-M curves.
Results
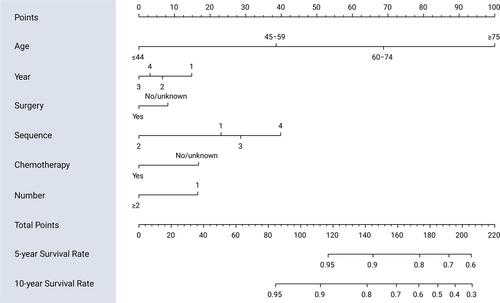
The major risk factors for cardiac death were age, surgery, year of diagnosis, sequence of surgery and radiotherapy, chemotherapy and a number of tumors, which were used to create the nomogram. The C-indexes of the nomograms were 0.708 and 0.679 for the development and validation groups, respectively. DCA showed the good net clinical benefit of nomograms in predicting 5- and 10-year risk of cardiac death. The model exhibited moderate predictive power for 5- and 10-year cardiac mortality (AUC: 0.833 and 0.854, respectively), and for the development and validation cohorts (AUC: 0.76 and 0.813, respectively).
Conclusions
Our nomogram may assist clinicians in making clinical decisions about patients undergoing radiotherapy for esophageal cancer based on early detection of cardiac death risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


