{"title":"导管依赖性肺循环中动脉导管支架置入后分支肺动脉狭窄的支架支架扩张。","authors":"Nageswara Rao Koneti, Shweta Bakhru, Bhargavi Dhulipudi, Saileela Rajan, Narayanswami Sreeram","doi":"10.1007/s00246-023-03319-2","DOIUrl":null,"url":null,"abstract":"<p><p>To assess the feasibility and outcome of stent strut dilation after arterial duct stenting with associated branch pulmonary artery (BPA) stenosis. Stenting of arterial duct in infants with duct-dependent pulmonary circulation is technically challenging. The presence of BPA stenosis is a relative contraindication for stent implantation. Infants with duct-dependent pulmonary circulation and associated BPA stenosis were assessed either by transthoracic echocardiogram alone or additional computerized tomography angiogram when required. Following ductal stenting, the stent struts of the stenosed BPA were crossed with an additional 0.014″ coronary guide wire and dilated using coronary balloons (2.0 or 2.5 mm in diameter). Seventeen (12 male) patients were considered for the procedure. The median age and weight were 27 days (range 2-94) and 2.6 kg (range 2.2-5), respectively. Fourteen patients (82.4%) underwent stent strut dilation after arterial duct stenting. Struts to left pulmonary artery was opened in 9 (64.3%) and right pulmonary artery in 5 (35.7%). The mean systemic oxygen saturation increased from 66.23 ± 8.9% at baseline to 86 ± 2.2% immediately after the stent deployment and final saturations after stent strut dilation were 89.29 ± 4.3%. Angiographic pulmonary flow improved in all cases. Stent strut dilation could not be done in 3 patients due to unfavorable anatomy. One patient had acute stent thrombosis and died in the hospital. Two others died during follow-up, during an acute febrile illness and gastroenteritis. All survivors underwent cardiac surgery and were on regular follow-up. Strut dilation of BPA stenosis is feasible to augment pulmonary blood flow, following arterial duct stenting. This procedure may be useful in selected patients with BPA stenosis to have uniform growth of pulmonary arteries.</p>","PeriodicalId":19814,"journal":{"name":"Pediatric Cardiology","volume":" ","pages":"53-60"},"PeriodicalIF":1.5000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Stent Strut Dilation in Branch Pulmonary Artery Stenosis Following Stenting of Arterial Duct in Duct-dependent Pulmonary Circulation.\",\"authors\":\"Nageswara Rao Koneti, Shweta Bakhru, Bhargavi Dhulipudi, Saileela Rajan, Narayanswami Sreeram\",\"doi\":\"10.1007/s00246-023-03319-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>To assess the feasibility and outcome of stent strut dilation after arterial duct stenting with associated branch pulmonary artery (BPA) stenosis. Stenting of arterial duct in infants with duct-dependent pulmonary circulation is technically challenging. The presence of BPA stenosis is a relative contraindication for stent implantation. Infants with duct-dependent pulmonary circulation and associated BPA stenosis were assessed either by transthoracic echocardiogram alone or additional computerized tomography angiogram when required. Following ductal stenting, the stent struts of the stenosed BPA were crossed with an additional 0.014″ coronary guide wire and dilated using coronary balloons (2.0 or 2.5 mm in diameter). Seventeen (12 male) patients were considered for the procedure. The median age and weight were 27 days (range 2-94) and 2.6 kg (range 2.2-5), respectively. Fourteen patients (82.4%) underwent stent strut dilation after arterial duct stenting. Struts to left pulmonary artery was opened in 9 (64.3%) and right pulmonary artery in 5 (35.7%). The mean systemic oxygen saturation increased from 66.23 ± 8.9% at baseline to 86 ± 2.2% immediately after the stent deployment and final saturations after stent strut dilation were 89.29 ± 4.3%. Angiographic pulmonary flow improved in all cases. Stent strut dilation could not be done in 3 patients due to unfavorable anatomy. One patient had acute stent thrombosis and died in the hospital. Two others died during follow-up, during an acute febrile illness and gastroenteritis. All survivors underwent cardiac surgery and were on regular follow-up. Strut dilation of BPA stenosis is feasible to augment pulmonary blood flow, following arterial duct stenting. This procedure may be useful in selected patients with BPA stenosis to have uniform growth of pulmonary arteries.</p>\",\"PeriodicalId\":19814,\"journal\":{\"name\":\"Pediatric Cardiology\",\"volume\":\" \",\"pages\":\"53-60\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00246-023-03319-2\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/11/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00246-023-03319-2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/6 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Stent Strut Dilation in Branch Pulmonary Artery Stenosis Following Stenting of Arterial Duct in Duct-dependent Pulmonary Circulation.
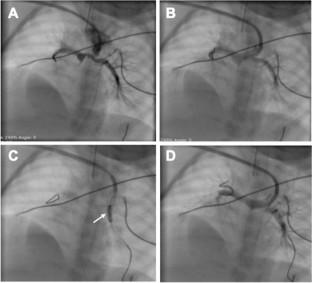
To assess the feasibility and outcome of stent strut dilation after arterial duct stenting with associated branch pulmonary artery (BPA) stenosis. Stenting of arterial duct in infants with duct-dependent pulmonary circulation is technically challenging. The presence of BPA stenosis is a relative contraindication for stent implantation. Infants with duct-dependent pulmonary circulation and associated BPA stenosis were assessed either by transthoracic echocardiogram alone or additional computerized tomography angiogram when required. Following ductal stenting, the stent struts of the stenosed BPA were crossed with an additional 0.014″ coronary guide wire and dilated using coronary balloons (2.0 or 2.5 mm in diameter). Seventeen (12 male) patients were considered for the procedure. The median age and weight were 27 days (range 2-94) and 2.6 kg (range 2.2-5), respectively. Fourteen patients (82.4%) underwent stent strut dilation after arterial duct stenting. Struts to left pulmonary artery was opened in 9 (64.3%) and right pulmonary artery in 5 (35.7%). The mean systemic oxygen saturation increased from 66.23 ± 8.9% at baseline to 86 ± 2.2% immediately after the stent deployment and final saturations after stent strut dilation were 89.29 ± 4.3%. Angiographic pulmonary flow improved in all cases. Stent strut dilation could not be done in 3 patients due to unfavorable anatomy. One patient had acute stent thrombosis and died in the hospital. Two others died during follow-up, during an acute febrile illness and gastroenteritis. All survivors underwent cardiac surgery and were on regular follow-up. Strut dilation of BPA stenosis is feasible to augment pulmonary blood flow, following arterial duct stenting. This procedure may be useful in selected patients with BPA stenosis to have uniform growth of pulmonary arteries.
期刊介绍:
The editor of Pediatric Cardiology welcomes original manuscripts concerning all aspects of heart disease in infants, children, and adolescents, including embryology and anatomy, physiology and pharmacology, biochemistry, pathology, genetics, radiology, clinical aspects, investigative cardiology, electrophysiology and echocardiography, and cardiac surgery. Articles which may include original articles, review articles, letters to the editor etc., must be written in English and must be submitted solely to Pediatric Cardiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


