{"title":"肾移植患者的De Novo纤维蛋白原Aα链淀粉样变性:病例报告和文献复习。","authors":"Taqui Khaja, Luan Truong, George Nassar","doi":"10.1177/20543581231209207","DOIUrl":null,"url":null,"abstract":"<p><strong>Rationale: </strong><i>De Novo</i> transplant amyloidosis denotes the condition when a patient develops amyloidosis after transplantation but had not been diagnosed with the disease prior to transplantation. The incidence of <i>de novo</i> amyloidosis in kidney transplants is rare, but few published case reports have described the occurrence of <i>de novo</i> Amyloid A protein (AA) and Light Chain (AL) amyloidosis. However, <i>de novo</i> hereditary fibrinogen A alpha chain (AFib) has not been previously reported.</p><p><strong>Patient presentation: </strong>We present a 72-year-old man, a kidney transplant recipient, who developed progressive rise in his creatinine about 3 years after transplantation. He has long-standing diabetes mellitus type 2, obesity, and hypertension, so he did not have a kidney biopsy of his native kidneys prior to transplantation.</p><p><strong>Diagnosis: </strong>A kidney transplant biopsy was done that showed amyloidosis. Mass spectrophotometry confirmed it as AFib amyloidosis. Genetic testing of the patient revealed that he has fibrinogen A alpha gene (FGA) point mutation with a p.E545V variant.</p><p><strong>Interventions: </strong>Cardiac evaluation showed normal transthoracic echocardiogram. Cardiac magnetic resonance imaging (MRI) showed no involvement by amyloidosis. A peripheral nerve biopsy showed diabetic neuropathy. Thus, the kidney was the only organ involved by the disease. The kidney transplant was managed conservatively with blood pressure and diabetes control in addition to his usual immunosuppression regimen which was not altered. He is being treated with diuretics, angiotensin receptor inhibitors, and sodium glucose transport 2 inhibitors.</p><p><strong>Outcomes: </strong>Kidney transplant function exhibited only slow progression over 18 months since the diagnosis was confirmed. This slow progression is likely because the p.E545V point mutation variant is less aggressive than other gene deletion mutations and because our patient was judged to have been diagnosed early in the course of his disease.</p><p><strong>Teaching points: </strong>In this case report, we illustrate the findings and testing that confirmed the diagnosis of AFib amyloidosis. We summarize the clinical aspects, outcomes of the disease, and treatment options. We believe this case report is interesting because it is the first reported case of AFib amyloidosis in a kidney transplant recipient who was not known to have the disease prior to kidney transplantation.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"10 ","pages":"20543581231209207"},"PeriodicalIF":1.6000,"publicationDate":"2023-10-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10619347/pdf/","citationCount":"0","resultStr":"{\"title\":\"De Novo Fibrinogen A Alpha Chain Amyloidosis in a Kidney Transplant Patient: Case Report and Literature Review.\",\"authors\":\"Taqui Khaja, Luan Truong, George Nassar\",\"doi\":\"10.1177/20543581231209207\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Rationale: </strong><i>De Novo</i> transplant amyloidosis denotes the condition when a patient develops amyloidosis after transplantation but had not been diagnosed with the disease prior to transplantation. The incidence of <i>de novo</i> amyloidosis in kidney transplants is rare, but few published case reports have described the occurrence of <i>de novo</i> Amyloid A protein (AA) and Light Chain (AL) amyloidosis. However, <i>de novo</i> hereditary fibrinogen A alpha chain (AFib) has not been previously reported.</p><p><strong>Patient presentation: </strong>We present a 72-year-old man, a kidney transplant recipient, who developed progressive rise in his creatinine about 3 years after transplantation. He has long-standing diabetes mellitus type 2, obesity, and hypertension, so he did not have a kidney biopsy of his native kidneys prior to transplantation.</p><p><strong>Diagnosis: </strong>A kidney transplant biopsy was done that showed amyloidosis. Mass spectrophotometry confirmed it as AFib amyloidosis. Genetic testing of the patient revealed that he has fibrinogen A alpha gene (FGA) point mutation with a p.E545V variant.</p><p><strong>Interventions: </strong>Cardiac evaluation showed normal transthoracic echocardiogram. Cardiac magnetic resonance imaging (MRI) showed no involvement by amyloidosis. A peripheral nerve biopsy showed diabetic neuropathy. Thus, the kidney was the only organ involved by the disease. The kidney transplant was managed conservatively with blood pressure and diabetes control in addition to his usual immunosuppression regimen which was not altered. He is being treated with diuretics, angiotensin receptor inhibitors, and sodium glucose transport 2 inhibitors.</p><p><strong>Outcomes: </strong>Kidney transplant function exhibited only slow progression over 18 months since the diagnosis was confirmed. This slow progression is likely because the p.E545V point mutation variant is less aggressive than other gene deletion mutations and because our patient was judged to have been diagnosed early in the course of his disease.</p><p><strong>Teaching points: </strong>In this case report, we illustrate the findings and testing that confirmed the diagnosis of AFib amyloidosis. We summarize the clinical aspects, outcomes of the disease, and treatment options. We believe this case report is interesting because it is the first reported case of AFib amyloidosis in a kidney transplant recipient who was not known to have the disease prior to kidney transplantation.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"10 \",\"pages\":\"20543581231209207\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2023-10-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10619347/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581231209207\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581231209207","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
De Novo Fibrinogen A Alpha Chain Amyloidosis in a Kidney Transplant Patient: Case Report and Literature Review.
Rationale: De Novo transplant amyloidosis denotes the condition when a patient develops amyloidosis after transplantation but had not been diagnosed with the disease prior to transplantation. The incidence of de novo amyloidosis in kidney transplants is rare, but few published case reports have described the occurrence of de novo Amyloid A protein (AA) and Light Chain (AL) amyloidosis. However, de novo hereditary fibrinogen A alpha chain (AFib) has not been previously reported.
Patient presentation: We present a 72-year-old man, a kidney transplant recipient, who developed progressive rise in his creatinine about 3 years after transplantation. He has long-standing diabetes mellitus type 2, obesity, and hypertension, so he did not have a kidney biopsy of his native kidneys prior to transplantation.
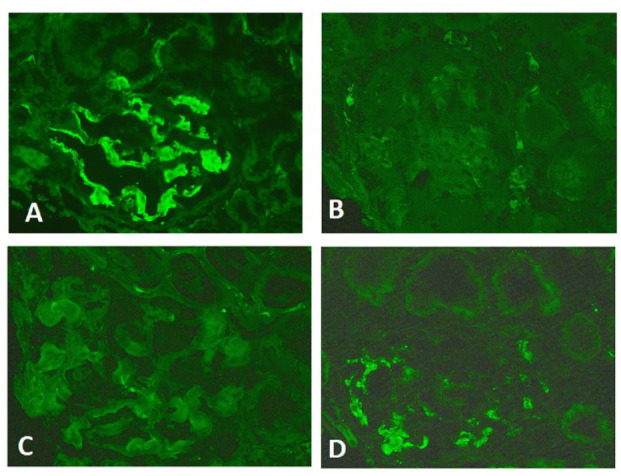
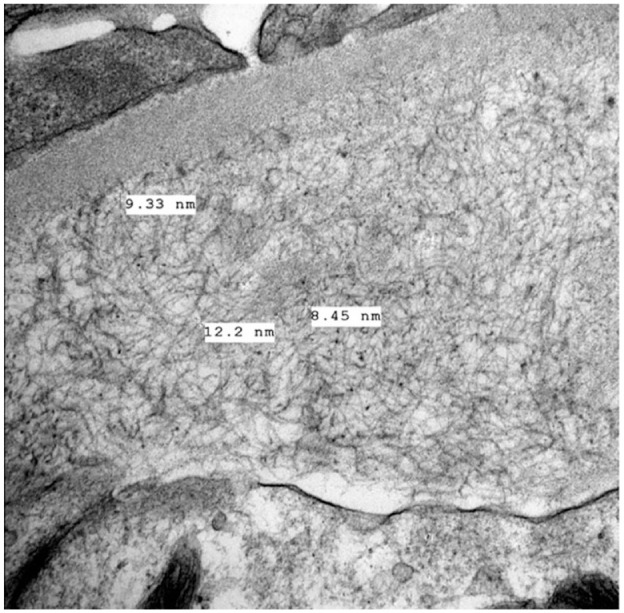
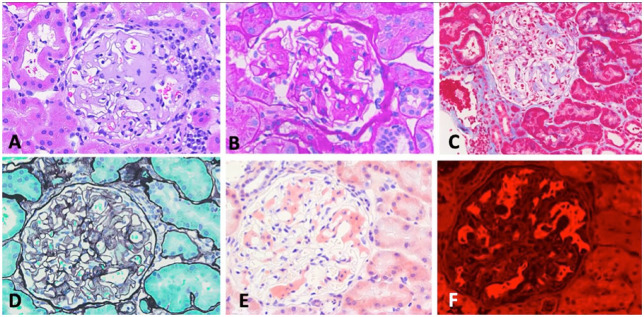
Diagnosis: A kidney transplant biopsy was done that showed amyloidosis. Mass spectrophotometry confirmed it as AFib amyloidosis. Genetic testing of the patient revealed that he has fibrinogen A alpha gene (FGA) point mutation with a p.E545V variant.
Interventions: Cardiac evaluation showed normal transthoracic echocardiogram. Cardiac magnetic resonance imaging (MRI) showed no involvement by amyloidosis. A peripheral nerve biopsy showed diabetic neuropathy. Thus, the kidney was the only organ involved by the disease. The kidney transplant was managed conservatively with blood pressure and diabetes control in addition to his usual immunosuppression regimen which was not altered. He is being treated with diuretics, angiotensin receptor inhibitors, and sodium glucose transport 2 inhibitors.
Outcomes: Kidney transplant function exhibited only slow progression over 18 months since the diagnosis was confirmed. This slow progression is likely because the p.E545V point mutation variant is less aggressive than other gene deletion mutations and because our patient was judged to have been diagnosed early in the course of his disease.
Teaching points: In this case report, we illustrate the findings and testing that confirmed the diagnosis of AFib amyloidosis. We summarize the clinical aspects, outcomes of the disease, and treatment options. We believe this case report is interesting because it is the first reported case of AFib amyloidosis in a kidney transplant recipient who was not known to have the disease prior to kidney transplantation.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


