Yusuf Sahin, Mehmet Yilmaz, Enes Kilic, Ahmet Yaser Muslumanoglu
{"title":"手术延迟增加经皮肾取石术围手术期输血率。","authors":"Yusuf Sahin, Mehmet Yilmaz, Enes Kilic, Ahmet Yaser Muslumanoglu","doi":"10.14744/SEMB.2023.63904","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>We aimed to investigate the effect of prolonged time from diagnosis to treatment (TDT) on surgical outcomes in patients undergoing percutaneous nephrolithotomy (PNL).</p><p><strong>Methods: </strong>This study included a total of 544 patients who underwent PNL in our clinic between November 2017 and November 2021. Clinicodemographical, radiological, and perioperative data of the patients were recorded. The stone-free rate as assessed by abdominal computed tomography at 3 months was estimated. The possible relation of the stone-free rate and perioperative complications with TDT was examined.</p><p><strong>Results: </strong>The median age was 48 (range, 38-58) years, the median stone size was 405 (range, 250-700) mm<sup>2</sup>, and the median stone density was 1,000 (range, 730-1,221) Hounsfield units. The median TDT was 75 (range, 42-133) days. Twenty-seven patients (5.0%) required perioperative blood transfusion (PBT). There was a statistically significant correlation between TDT and the need for PBT (p=0.022). However, there was no significant correlation between TDT and stone-free rate (p>0.05). Using a cutoff value of 90.5 days, TDT could predict the need for PBT with 59.3% sensitivity and 60% specificity.</p><p><strong>Conclusion: </strong>Our study results suggest that the need for PBT increases in patients undergoing PNL longer than 90.5 days after the diagnosis. However, further large-scale, prospective studies are warranted to elucidate the effect of prolonged TDT on surgical outcomes in this patient population.</p>","PeriodicalId":42218,"journal":{"name":"Medical Bulletin of Sisli Etfal Hospital","volume":null,"pages":null},"PeriodicalIF":1.0000,"publicationDate":"2023-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10600608/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical Delay Increases the Perioperative Blood Transfusion Rate In Percutaneous Nephrolithotomy.\",\"authors\":\"Yusuf Sahin, Mehmet Yilmaz, Enes Kilic, Ahmet Yaser Muslumanoglu\",\"doi\":\"10.14744/SEMB.2023.63904\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>We aimed to investigate the effect of prolonged time from diagnosis to treatment (TDT) on surgical outcomes in patients undergoing percutaneous nephrolithotomy (PNL).</p><p><strong>Methods: </strong>This study included a total of 544 patients who underwent PNL in our clinic between November 2017 and November 2021. Clinicodemographical, radiological, and perioperative data of the patients were recorded. The stone-free rate as assessed by abdominal computed tomography at 3 months was estimated. The possible relation of the stone-free rate and perioperative complications with TDT was examined.</p><p><strong>Results: </strong>The median age was 48 (range, 38-58) years, the median stone size was 405 (range, 250-700) mm<sup>2</sup>, and the median stone density was 1,000 (range, 730-1,221) Hounsfield units. The median TDT was 75 (range, 42-133) days. Twenty-seven patients (5.0%) required perioperative blood transfusion (PBT). There was a statistically significant correlation between TDT and the need for PBT (p=0.022). However, there was no significant correlation between TDT and stone-free rate (p>0.05). Using a cutoff value of 90.5 days, TDT could predict the need for PBT with 59.3% sensitivity and 60% specificity.</p><p><strong>Conclusion: </strong>Our study results suggest that the need for PBT increases in patients undergoing PNL longer than 90.5 days after the diagnosis. However, further large-scale, prospective studies are warranted to elucidate the effect of prolonged TDT on surgical outcomes in this patient population.</p>\",\"PeriodicalId\":42218,\"journal\":{\"name\":\"Medical Bulletin of Sisli Etfal Hospital\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2023-09-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10600608/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical Bulletin of Sisli Etfal Hospital\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14744/SEMB.2023.63904\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Bulletin of Sisli Etfal Hospital","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/SEMB.2023.63904","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Surgical Delay Increases the Perioperative Blood Transfusion Rate In Percutaneous Nephrolithotomy.
Objectives: We aimed to investigate the effect of prolonged time from diagnosis to treatment (TDT) on surgical outcomes in patients undergoing percutaneous nephrolithotomy (PNL).
Methods: This study included a total of 544 patients who underwent PNL in our clinic between November 2017 and November 2021. Clinicodemographical, radiological, and perioperative data of the patients were recorded. The stone-free rate as assessed by abdominal computed tomography at 3 months was estimated. The possible relation of the stone-free rate and perioperative complications with TDT was examined.
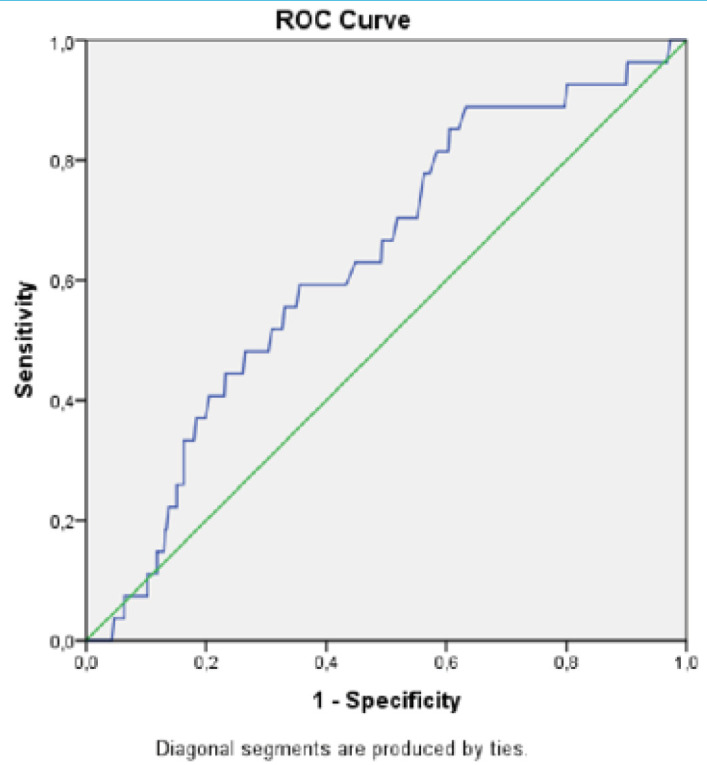
Results: The median age was 48 (range, 38-58) years, the median stone size was 405 (range, 250-700) mm2, and the median stone density was 1,000 (range, 730-1,221) Hounsfield units. The median TDT was 75 (range, 42-133) days. Twenty-seven patients (5.0%) required perioperative blood transfusion (PBT). There was a statistically significant correlation between TDT and the need for PBT (p=0.022). However, there was no significant correlation between TDT and stone-free rate (p>0.05). Using a cutoff value of 90.5 days, TDT could predict the need for PBT with 59.3% sensitivity and 60% specificity.
Conclusion: Our study results suggest that the need for PBT increases in patients undergoing PNL longer than 90.5 days after the diagnosis. However, further large-scale, prospective studies are warranted to elucidate the effect of prolonged TDT on surgical outcomes in this patient population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


