Nitish Sood, Anish Sangari, Arnav Goyal, Christina Sun, Madison Horinek, Joseph Andy Hauger, Lane Perry
{"title":"心肺复苏实时视听反馈设备能改善患者的预后吗?系统综述和荟萃分析。","authors":"Nitish Sood, Anish Sangari, Arnav Goyal, Christina Sun, Madison Horinek, Joseph Andy Hauger, Lane Perry","doi":"10.4330/wjc.v15.i10.531","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiac arrest is a leading cause of mortality in America and has increased in the incidence of cases over the last several years. Cardiopulmonary resuscitation (CPR) increases survival outcomes in cases of cardiac arrest; however, healthcare workers often do not perform CPR within recommended guidelines. Real-time audiovisual feedback (RTAVF) devices improve the quality of CPR performed. This systematic review and meta-analysis aims to compare the effect of RTAVF-assisted CPR with conventional CPR and to evaluate whether the use of these devices improved outcomes in both in-hospital cardiac arrest (IHCA) and out-of-hospital cardiac arrest (OHCA) patients.</p><p><strong>Aim: </strong>To identify the effect of RTAVF-assisted CPR on patient outcomes and CPR quality with in- and OHCA.</p><p><strong>Methods: </strong>We searched PubMed, SCOPUS, the Cochrane Library, and EMBASE from inception to July 27, 2020, for studies comparing patient outcomes and/or CPR quality metrics between RTAVF-assisted CPR and conventional CPR in cases of IHCA or OHCA. The primary outcomes of interest were return of spontaneous circulation (ROSC) and survival to hospital discharge (SHD), with secondary outcomes of chest compression rate and chest compression depth. The methodological quality of the included studies was assessed using the Newcastle-Ottawa scale and Cochrane Collaboration's \"risk of bias\" tool. Data was analyzed using R statistical software 4.2.0. results were statistically significant if <i>P</i> < 0.05.</p><p><strong>Results: </strong>Thirteen studies (<i>n</i> = 17600) were included. Patients were on average 69 ± 17.5 years old, with 7022 (39.8%) female patients. Overall pooled ROSC in patients in this study was 37% (95% confidence interval = 23%-54%). RTAVF-assisted CPR significantly improved ROSC, both overall [risk ratio (RR) 1.17 (1.001-1.362); <i>P</i> = 0.048] and in cases of IHCA [RR 1.36 (1.06-1.80); <i>P</i> = 0.002]. There was no significant improvement in ROSC for OHCA (RR 1.04; 0.91-1.19; <i>P</i> = 0.47). No significant effect was seen in SHD [RR 1.04 (0.91-1.19); <i>P</i> = 0.47] or chest compression rate [standardized mean difference (SMD) -2.1; (-4.6-0.5)]; <i>P</i> = 0.09]. A significant improvement was seen in chest compression depth [SMD 1.6; (0.02-3.1); <i>P</i> = 0.047].</p><p><strong>Conclusion: </strong>RTAVF-assisted CPR increases ROSC in cases of IHCA and chest compression depth but has no significant effect on ROSC in cases of OHCA, SHD, or chest compression rate.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":"15 10","pages":"531-541"},"PeriodicalIF":1.9000,"publicationDate":"2023-10-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10600786/pdf/","citationCount":"0","resultStr":"{\"title\":\"Do cardiopulmonary resuscitation real-time audiovisual feedback devices improve patient outcomes? A systematic review and meta-analysis.\",\"authors\":\"Nitish Sood, Anish Sangari, Arnav Goyal, Christina Sun, Madison Horinek, Joseph Andy Hauger, Lane Perry\",\"doi\":\"10.4330/wjc.v15.i10.531\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiac arrest is a leading cause of mortality in America and has increased in the incidence of cases over the last several years. Cardiopulmonary resuscitation (CPR) increases survival outcomes in cases of cardiac arrest; however, healthcare workers often do not perform CPR within recommended guidelines. Real-time audiovisual feedback (RTAVF) devices improve the quality of CPR performed. This systematic review and meta-analysis aims to compare the effect of RTAVF-assisted CPR with conventional CPR and to evaluate whether the use of these devices improved outcomes in both in-hospital cardiac arrest (IHCA) and out-of-hospital cardiac arrest (OHCA) patients.</p><p><strong>Aim: </strong>To identify the effect of RTAVF-assisted CPR on patient outcomes and CPR quality with in- and OHCA.</p><p><strong>Methods: </strong>We searched PubMed, SCOPUS, the Cochrane Library, and EMBASE from inception to July 27, 2020, for studies comparing patient outcomes and/or CPR quality metrics between RTAVF-assisted CPR and conventional CPR in cases of IHCA or OHCA. The primary outcomes of interest were return of spontaneous circulation (ROSC) and survival to hospital discharge (SHD), with secondary outcomes of chest compression rate and chest compression depth. The methodological quality of the included studies was assessed using the Newcastle-Ottawa scale and Cochrane Collaboration's \\\"risk of bias\\\" tool. Data was analyzed using R statistical software 4.2.0. results were statistically significant if <i>P</i> < 0.05.</p><p><strong>Results: </strong>Thirteen studies (<i>n</i> = 17600) were included. Patients were on average 69 ± 17.5 years old, with 7022 (39.8%) female patients. Overall pooled ROSC in patients in this study was 37% (95% confidence interval = 23%-54%). RTAVF-assisted CPR significantly improved ROSC, both overall [risk ratio (RR) 1.17 (1.001-1.362); <i>P</i> = 0.048] and in cases of IHCA [RR 1.36 (1.06-1.80); <i>P</i> = 0.002]. There was no significant improvement in ROSC for OHCA (RR 1.04; 0.91-1.19; <i>P</i> = 0.47). No significant effect was seen in SHD [RR 1.04 (0.91-1.19); <i>P</i> = 0.47] or chest compression rate [standardized mean difference (SMD) -2.1; (-4.6-0.5)]; <i>P</i> = 0.09]. A significant improvement was seen in chest compression depth [SMD 1.6; (0.02-3.1); <i>P</i> = 0.047].</p><p><strong>Conclusion: </strong>RTAVF-assisted CPR increases ROSC in cases of IHCA and chest compression depth but has no significant effect on ROSC in cases of OHCA, SHD, or chest compression rate.</p>\",\"PeriodicalId\":23800,\"journal\":{\"name\":\"World Journal of Cardiology\",\"volume\":\"15 10\",\"pages\":\"531-541\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2023-10-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10600786/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4330/wjc.v15.i10.531\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v15.i10.531","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Do cardiopulmonary resuscitation real-time audiovisual feedback devices improve patient outcomes? A systematic review and meta-analysis.
Background: Cardiac arrest is a leading cause of mortality in America and has increased in the incidence of cases over the last several years. Cardiopulmonary resuscitation (CPR) increases survival outcomes in cases of cardiac arrest; however, healthcare workers often do not perform CPR within recommended guidelines. Real-time audiovisual feedback (RTAVF) devices improve the quality of CPR performed. This systematic review and meta-analysis aims to compare the effect of RTAVF-assisted CPR with conventional CPR and to evaluate whether the use of these devices improved outcomes in both in-hospital cardiac arrest (IHCA) and out-of-hospital cardiac arrest (OHCA) patients.
Aim: To identify the effect of RTAVF-assisted CPR on patient outcomes and CPR quality with in- and OHCA.
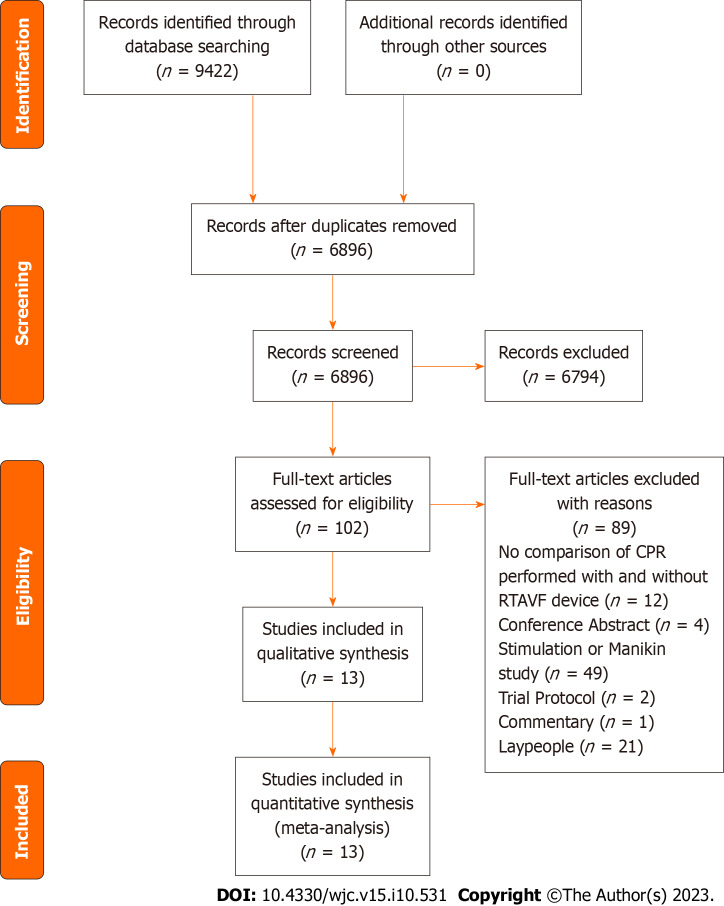
Methods: We searched PubMed, SCOPUS, the Cochrane Library, and EMBASE from inception to July 27, 2020, for studies comparing patient outcomes and/or CPR quality metrics between RTAVF-assisted CPR and conventional CPR in cases of IHCA or OHCA. The primary outcomes of interest were return of spontaneous circulation (ROSC) and survival to hospital discharge (SHD), with secondary outcomes of chest compression rate and chest compression depth. The methodological quality of the included studies was assessed using the Newcastle-Ottawa scale and Cochrane Collaboration's "risk of bias" tool. Data was analyzed using R statistical software 4.2.0. results were statistically significant if P < 0.05.
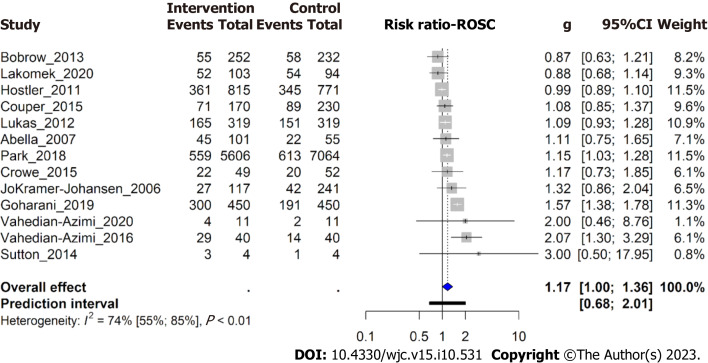
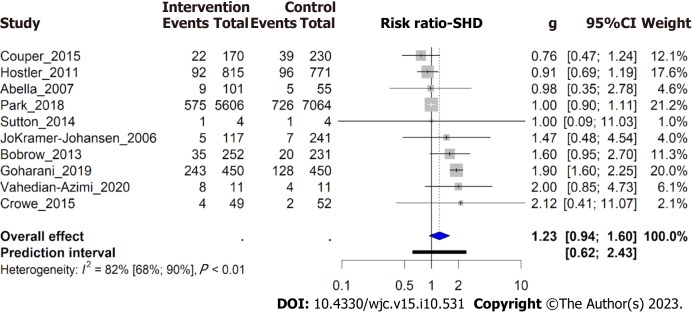
Results: Thirteen studies (n = 17600) were included. Patients were on average 69 ± 17.5 years old, with 7022 (39.8%) female patients. Overall pooled ROSC in patients in this study was 37% (95% confidence interval = 23%-54%). RTAVF-assisted CPR significantly improved ROSC, both overall [risk ratio (RR) 1.17 (1.001-1.362); P = 0.048] and in cases of IHCA [RR 1.36 (1.06-1.80); P = 0.002]. There was no significant improvement in ROSC for OHCA (RR 1.04; 0.91-1.19; P = 0.47). No significant effect was seen in SHD [RR 1.04 (0.91-1.19); P = 0.47] or chest compression rate [standardized mean difference (SMD) -2.1; (-4.6-0.5)]; P = 0.09]. A significant improvement was seen in chest compression depth [SMD 1.6; (0.02-3.1); P = 0.047].
Conclusion: RTAVF-assisted CPR increases ROSC in cases of IHCA and chest compression depth but has no significant effect on ROSC in cases of OHCA, SHD, or chest compression rate.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


