Jakob Lillemoen Drivenes, Mette Ramsing, Anette Bygum
{"title":"Majocchi氏肉芽肿——大咪咪:一例报告。","authors":"Jakob Lillemoen Drivenes, Mette Ramsing, Anette Bygum","doi":"10.1159/000533475","DOIUrl":null,"url":null,"abstract":"<p><p>Fungal infections can be challenging to diagnose, but doctors of every specialty may encounter this issue. They can be mistaken for other common dermatoses such as eczema or psoriasis and inadvertently be treated with topical corticosteroids or calcineurin inhibitors. This may lead to tinea incognita, a term used to describe a fungal infection with an altered clinical appearance, which may confuse the clinician even further. This case report presents a 54-year-old previously healthy man with a 4-month history of a painful and pruritic rash in the genitoinguinal region. The patient's general practitioner had unsuccessfully attempted to treat the rash with topical terbinafine, econazole-triamcinolone, and betamethasone-fusidic acid, in addition to peroral dicloxacillin capsules. On examination, there were multiple red-bluish nodules and pustules coalescing into infiltrating erythematous plaques on both thighs and in the pubic region. Fungal cultures were negative, but the clinical features together with the history of prolonged use of combined topical steroids and antifungals raised suspicion of a deep fungal infection. Histopathological skin examination revealed deep suppurative and granulomatous folliculitis with ruptured hair follicles which was consistent with a diagnosis of Majocchi's granuloma. Treatment with itraconazole capsules was initiated, and after a 16-week course of systemic antifungal therapy, the rash resolved. In conclusion, our case report presents a case of Majocchi's granuloma, which is a great mimicker, especially for non-dermatologists. It is therefore important that the diagnosis is considered as a differential diagnosis, even though a patient has previously been treated with a topical antifungal.</p>","PeriodicalId":9619,"journal":{"name":"Case Reports in Dermatology","volume":"15 1","pages":"190-193"},"PeriodicalIF":0.8000,"publicationDate":"2023-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10601710/pdf/","citationCount":"0","resultStr":"{\"title\":\"Majocchi's Granuloma - The Great Mimicker: A Case Report.\",\"authors\":\"Jakob Lillemoen Drivenes, Mette Ramsing, Anette Bygum\",\"doi\":\"10.1159/000533475\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Fungal infections can be challenging to diagnose, but doctors of every specialty may encounter this issue. They can be mistaken for other common dermatoses such as eczema or psoriasis and inadvertently be treated with topical corticosteroids or calcineurin inhibitors. This may lead to tinea incognita, a term used to describe a fungal infection with an altered clinical appearance, which may confuse the clinician even further. This case report presents a 54-year-old previously healthy man with a 4-month history of a painful and pruritic rash in the genitoinguinal region. The patient's general practitioner had unsuccessfully attempted to treat the rash with topical terbinafine, econazole-triamcinolone, and betamethasone-fusidic acid, in addition to peroral dicloxacillin capsules. On examination, there were multiple red-bluish nodules and pustules coalescing into infiltrating erythematous plaques on both thighs and in the pubic region. Fungal cultures were negative, but the clinical features together with the history of prolonged use of combined topical steroids and antifungals raised suspicion of a deep fungal infection. Histopathological skin examination revealed deep suppurative and granulomatous folliculitis with ruptured hair follicles which was consistent with a diagnosis of Majocchi's granuloma. Treatment with itraconazole capsules was initiated, and after a 16-week course of systemic antifungal therapy, the rash resolved. In conclusion, our case report presents a case of Majocchi's granuloma, which is a great mimicker, especially for non-dermatologists. It is therefore important that the diagnosis is considered as a differential diagnosis, even though a patient has previously been treated with a topical antifungal.</p>\",\"PeriodicalId\":9619,\"journal\":{\"name\":\"Case Reports in Dermatology\",\"volume\":\"15 1\",\"pages\":\"190-193\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-10-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10601710/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Dermatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000533475\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Dermatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000533475","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"DERMATOLOGY","Score":null,"Total":0}
Majocchi's Granuloma - The Great Mimicker: A Case Report.
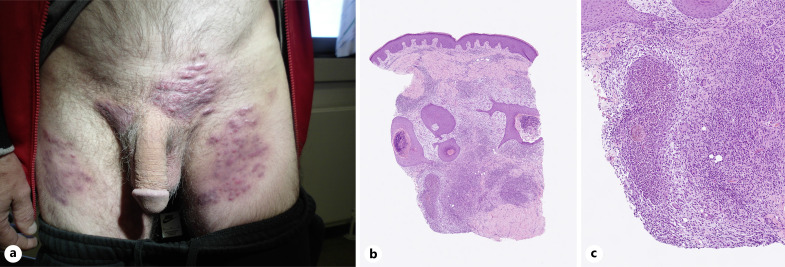
Fungal infections can be challenging to diagnose, but doctors of every specialty may encounter this issue. They can be mistaken for other common dermatoses such as eczema or psoriasis and inadvertently be treated with topical corticosteroids or calcineurin inhibitors. This may lead to tinea incognita, a term used to describe a fungal infection with an altered clinical appearance, which may confuse the clinician even further. This case report presents a 54-year-old previously healthy man with a 4-month history of a painful and pruritic rash in the genitoinguinal region. The patient's general practitioner had unsuccessfully attempted to treat the rash with topical terbinafine, econazole-triamcinolone, and betamethasone-fusidic acid, in addition to peroral dicloxacillin capsules. On examination, there were multiple red-bluish nodules and pustules coalescing into infiltrating erythematous plaques on both thighs and in the pubic region. Fungal cultures were negative, but the clinical features together with the history of prolonged use of combined topical steroids and antifungals raised suspicion of a deep fungal infection. Histopathological skin examination revealed deep suppurative and granulomatous folliculitis with ruptured hair follicles which was consistent with a diagnosis of Majocchi's granuloma. Treatment with itraconazole capsules was initiated, and after a 16-week course of systemic antifungal therapy, the rash resolved. In conclusion, our case report presents a case of Majocchi's granuloma, which is a great mimicker, especially for non-dermatologists. It is therefore important that the diagnosis is considered as a differential diagnosis, even though a patient has previously been treated with a topical antifungal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


