Eric M Bomberg, Elise F Palzer, Kyle D Rudser, Aaron S Kelly, Carolyn T Bramante, Hilary K Seligman, Favour Noni, Claudia K Fox
{"title":"按种族/民族分列的抗肥胖药物处方以及儿科体重管理诊所使用翻译的情况。","authors":"Eric M Bomberg, Elise F Palzer, Kyle D Rudser, Aaron S Kelly, Carolyn T Bramante, Hilary K Seligman, Favour Noni, Claudia K Fox","doi":"10.1177/20420188221090009","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Race/ethnicity and low English proficiency healthcare disparities are well established in the United States. We sought to determine if there are race/ethnicity differences in anti-obesity medication (AOM) prescription rates among youth with severe obesity treated in a pediatric weight management clinic and if, among youth from non-primary English speaking families, there are differences in prescriptions between those using interpreters during visits versus not.</p><p><strong>Methods: </strong>We reviewed electronic health records of 2- to 18-year-olds with severe obesity seen from 2012 to 2021. Race/ethnicity was self-report, and AOMs included topiramate, stimulants (e.g. phentermine, lisdexamfetamine), naltrexone (±bupropion), glucagon-like peptide-1 agonists, and orlistat. We used general linear regression models with log-link to compare incidence rate ratios (IRRs) within the first 1 and 3 years of being followed, controlling for age, percent of the 95th BMI percentile (%BMIp95), number of obesity-related comorbidities (e.g. insulin resistance, hypertension), median household income, and interpreter use. We repeated similar analyses among youth from non-primary English speaking families, comparing those using interpreters versus not.</p><p><strong>Results: </strong>1,725 youth (mean age 11.5 years; %BMIp95 142%; 53% non-Hispanic White, 20% Hispanic/Latino, 16% non-Hispanic black; 6% used interpreters) were seen, of which 15% were prescribed AOMs within 1 year. The IRR for prescriptions was lower among Hispanic/Latino compared to non-Hispanic White youth at one (IRR 0.70; CI: 0.49-1.00; <i>p</i> = 0.047) but not 3 years. No other statistically significant differences by race/ethnicity were found. Among non-primary English speaking families, the IRR for prescriptions was higher at 1 year (IRR 2.49; CI: 1.32-4.70; <i>p</i> = 0.005) in those using interpreters versus not.</p><p><strong>Conclusions: </strong>Among youth seen in a pediatric weight management clinic, AOM prescription incidence rates were lower in Hispanics/Latinos compared to non-Hispanic Whites. Interpreter use was associated with higher prescription incidence rates among non-primary English speakers. Interventions to achieve equity in AOM prescriptions may help mitigate disparities in pediatric obesity.</p>","PeriodicalId":22998,"journal":{"name":"Therapeutic Advances in Endocrinology and Metabolism","volume":"13 1","pages":"20420188221090009"},"PeriodicalIF":4.6000,"publicationDate":"2022-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9005816/pdf/","citationCount":"0","resultStr":"{\"title\":\"Anti-obesity medication prescriptions by race/ethnicity and use of an interpreter in a pediatric weight management clinic.\",\"authors\":\"Eric M Bomberg, Elise F Palzer, Kyle D Rudser, Aaron S Kelly, Carolyn T Bramante, Hilary K Seligman, Favour Noni, Claudia K Fox\",\"doi\":\"10.1177/20420188221090009\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Race/ethnicity and low English proficiency healthcare disparities are well established in the United States. We sought to determine if there are race/ethnicity differences in anti-obesity medication (AOM) prescription rates among youth with severe obesity treated in a pediatric weight management clinic and if, among youth from non-primary English speaking families, there are differences in prescriptions between those using interpreters during visits versus not.</p><p><strong>Methods: </strong>We reviewed electronic health records of 2- to 18-year-olds with severe obesity seen from 2012 to 2021. Race/ethnicity was self-report, and AOMs included topiramate, stimulants (e.g. phentermine, lisdexamfetamine), naltrexone (±bupropion), glucagon-like peptide-1 agonists, and orlistat. We used general linear regression models with log-link to compare incidence rate ratios (IRRs) within the first 1 and 3 years of being followed, controlling for age, percent of the 95th BMI percentile (%BMIp95), number of obesity-related comorbidities (e.g. insulin resistance, hypertension), median household income, and interpreter use. We repeated similar analyses among youth from non-primary English speaking families, comparing those using interpreters versus not.</p><p><strong>Results: </strong>1,725 youth (mean age 11.5 years; %BMIp95 142%; 53% non-Hispanic White, 20% Hispanic/Latino, 16% non-Hispanic black; 6% used interpreters) were seen, of which 15% were prescribed AOMs within 1 year. The IRR for prescriptions was lower among Hispanic/Latino compared to non-Hispanic White youth at one (IRR 0.70; CI: 0.49-1.00; <i>p</i> = 0.047) but not 3 years. No other statistically significant differences by race/ethnicity were found. Among non-primary English speaking families, the IRR for prescriptions was higher at 1 year (IRR 2.49; CI: 1.32-4.70; <i>p</i> = 0.005) in those using interpreters versus not.</p><p><strong>Conclusions: </strong>Among youth seen in a pediatric weight management clinic, AOM prescription incidence rates were lower in Hispanics/Latinos compared to non-Hispanic Whites. Interpreter use was associated with higher prescription incidence rates among non-primary English speakers. Interventions to achieve equity in AOM prescriptions may help mitigate disparities in pediatric obesity.</p>\",\"PeriodicalId\":22998,\"journal\":{\"name\":\"Therapeutic Advances in Endocrinology and Metabolism\",\"volume\":\"13 1\",\"pages\":\"20420188221090009\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2022-04-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9005816/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Endocrinology and Metabolism\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/20420188221090009\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Endocrinology and Metabolism","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420188221090009","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Anti-obesity medication prescriptions by race/ethnicity and use of an interpreter in a pediatric weight management clinic.
Background: Race/ethnicity and low English proficiency healthcare disparities are well established in the United States. We sought to determine if there are race/ethnicity differences in anti-obesity medication (AOM) prescription rates among youth with severe obesity treated in a pediatric weight management clinic and if, among youth from non-primary English speaking families, there are differences in prescriptions between those using interpreters during visits versus not.
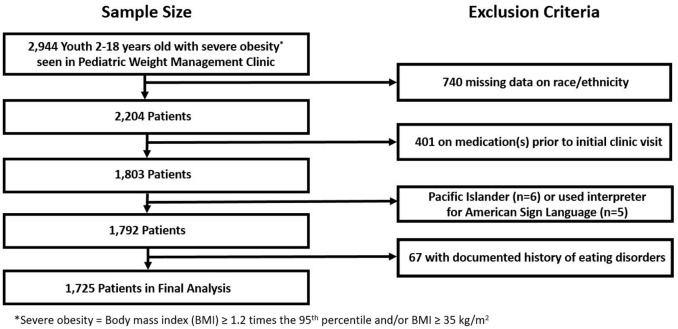
Methods: We reviewed electronic health records of 2- to 18-year-olds with severe obesity seen from 2012 to 2021. Race/ethnicity was self-report, and AOMs included topiramate, stimulants (e.g. phentermine, lisdexamfetamine), naltrexone (±bupropion), glucagon-like peptide-1 agonists, and orlistat. We used general linear regression models with log-link to compare incidence rate ratios (IRRs) within the first 1 and 3 years of being followed, controlling for age, percent of the 95th BMI percentile (%BMIp95), number of obesity-related comorbidities (e.g. insulin resistance, hypertension), median household income, and interpreter use. We repeated similar analyses among youth from non-primary English speaking families, comparing those using interpreters versus not.
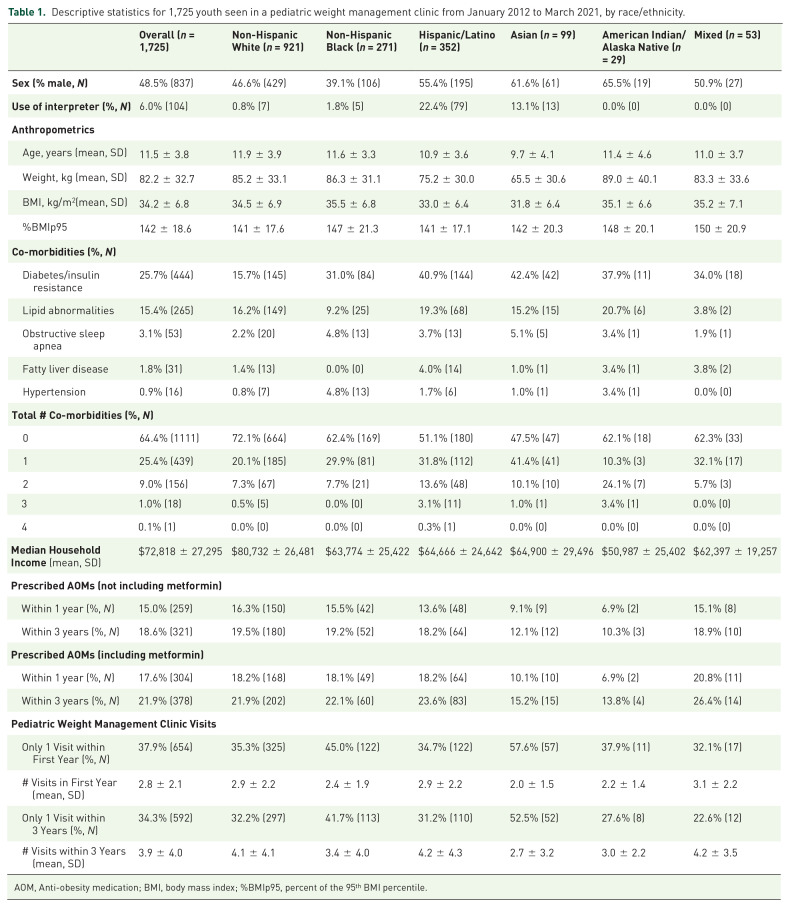
Results: 1,725 youth (mean age 11.5 years; %BMIp95 142%; 53% non-Hispanic White, 20% Hispanic/Latino, 16% non-Hispanic black; 6% used interpreters) were seen, of which 15% were prescribed AOMs within 1 year. The IRR for prescriptions was lower among Hispanic/Latino compared to non-Hispanic White youth at one (IRR 0.70; CI: 0.49-1.00; p = 0.047) but not 3 years. No other statistically significant differences by race/ethnicity were found. Among non-primary English speaking families, the IRR for prescriptions was higher at 1 year (IRR 2.49; CI: 1.32-4.70; p = 0.005) in those using interpreters versus not.
Conclusions: Among youth seen in a pediatric weight management clinic, AOM prescription incidence rates were lower in Hispanics/Latinos compared to non-Hispanic Whites. Interpreter use was associated with higher prescription incidence rates among non-primary English speakers. Interventions to achieve equity in AOM prescriptions may help mitigate disparities in pediatric obesity.
期刊介绍:
Therapeutic Advances in Endocrinology and Metabolism delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of endocrinology and metabolism.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


