{"title":"SAPHO综合征:目前的临床、诊断和治疗方法。","authors":"Tuba Demirci Yildirim, İsmail Sari","doi":"10.1007/s00296-023-05491-3","DOIUrl":null,"url":null,"abstract":"<p><p>This review provides an overview of SAPHO (Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis), a rare autoinflammatory disease that primarily affects bones, skin, and joints. We conducted a search on Medline/PubMed using keywords such as SAPHO syndrome, chronic recurrent multifocal osteitis/osteomyelitis, and related terms. SAPHO syndrome is rare, with a reported frequency of 1 in 10,000 in the Caucasian population. However, the actual incidence of SAPHO syndrome is unknown, and the incidence of the disease is likely higher. The pathogenesis of SAPHO syndrome remains incompletely understood. Current evidence suggests that SAPHO results from a complex interplay between immune dysregulation, genetic susceptibility, and environmental factors. It's not clear if SAPHO syndrome is an autoimmune disease or an autoinflammatory disease, but current evidence suggests that it's more likely an autoinflammatory disease because of things like neutrophil hyperactivity, fewer natural killer (NK) cells, high levels of interleukin (IL)-1, and a good response to treatments that block IL-1. Osteo-articular (OA) involvement is a key clinical feature of SAPHO. It affects the anterior chest wall, axial skeleton, peripheral joints, mandible, long bones of the extremities, and pelvis. Dermatological involvement is a common target in SAPHO, with lesions observed in 60-90% of cases. Common skin lesions include psoriasis and acne, with hidradenitis suppurativa and neutrophilic dermatoses being less commonly seen. Other clinical findings include constitutional symptoms caused by systemic inflammation, such as fever, weight loss, and fatigue. There is no specific laboratory finding for SAPHO syndrome. However, during active disease, there may be an increase in positive acute phase markers, such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), complement levels, mild leukocytosis, and thrombocytosis. Diagnosis is crucial for SAPHO syndrome, which lacks a specific diagnostic finding and is often underrecognized. A comprehensive evaluation of a patient's medical history and physical examination is crucial. Treatment options include non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, conventional and synthetic disease-modifying agents (cDMARDs and sDMARDs), biological therapies, bisphosphonates, and antibiotics. Biological treatments have emerged as a viable alternative for SAPHO patients who do not respond to conventional treatments.</p>","PeriodicalId":21322,"journal":{"name":"Rheumatology International","volume":" ","pages":"2301-2313"},"PeriodicalIF":2.9000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"SAPHO syndrome: current clinical, diagnostic and treatment approaches.\",\"authors\":\"Tuba Demirci Yildirim, İsmail Sari\",\"doi\":\"10.1007/s00296-023-05491-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>This review provides an overview of SAPHO (Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis), a rare autoinflammatory disease that primarily affects bones, skin, and joints. We conducted a search on Medline/PubMed using keywords such as SAPHO syndrome, chronic recurrent multifocal osteitis/osteomyelitis, and related terms. SAPHO syndrome is rare, with a reported frequency of 1 in 10,000 in the Caucasian population. However, the actual incidence of SAPHO syndrome is unknown, and the incidence of the disease is likely higher. The pathogenesis of SAPHO syndrome remains incompletely understood. Current evidence suggests that SAPHO results from a complex interplay between immune dysregulation, genetic susceptibility, and environmental factors. It's not clear if SAPHO syndrome is an autoimmune disease or an autoinflammatory disease, but current evidence suggests that it's more likely an autoinflammatory disease because of things like neutrophil hyperactivity, fewer natural killer (NK) cells, high levels of interleukin (IL)-1, and a good response to treatments that block IL-1. Osteo-articular (OA) involvement is a key clinical feature of SAPHO. It affects the anterior chest wall, axial skeleton, peripheral joints, mandible, long bones of the extremities, and pelvis. Dermatological involvement is a common target in SAPHO, with lesions observed in 60-90% of cases. Common skin lesions include psoriasis and acne, with hidradenitis suppurativa and neutrophilic dermatoses being less commonly seen. Other clinical findings include constitutional symptoms caused by systemic inflammation, such as fever, weight loss, and fatigue. There is no specific laboratory finding for SAPHO syndrome. However, during active disease, there may be an increase in positive acute phase markers, such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), complement levels, mild leukocytosis, and thrombocytosis. Diagnosis is crucial for SAPHO syndrome, which lacks a specific diagnostic finding and is often underrecognized. A comprehensive evaluation of a patient's medical history and physical examination is crucial. Treatment options include non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, conventional and synthetic disease-modifying agents (cDMARDs and sDMARDs), biological therapies, bisphosphonates, and antibiotics. Biological treatments have emerged as a viable alternative for SAPHO patients who do not respond to conventional treatments.</p>\",\"PeriodicalId\":21322,\"journal\":{\"name\":\"Rheumatology International\",\"volume\":\" \",\"pages\":\"2301-2313\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rheumatology International\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00296-023-05491-3\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rheumatology International","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00296-023-05491-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
SAPHO syndrome: current clinical, diagnostic and treatment approaches.
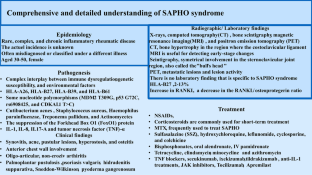
This review provides an overview of SAPHO (Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis), a rare autoinflammatory disease that primarily affects bones, skin, and joints. We conducted a search on Medline/PubMed using keywords such as SAPHO syndrome, chronic recurrent multifocal osteitis/osteomyelitis, and related terms. SAPHO syndrome is rare, with a reported frequency of 1 in 10,000 in the Caucasian population. However, the actual incidence of SAPHO syndrome is unknown, and the incidence of the disease is likely higher. The pathogenesis of SAPHO syndrome remains incompletely understood. Current evidence suggests that SAPHO results from a complex interplay between immune dysregulation, genetic susceptibility, and environmental factors. It's not clear if SAPHO syndrome is an autoimmune disease or an autoinflammatory disease, but current evidence suggests that it's more likely an autoinflammatory disease because of things like neutrophil hyperactivity, fewer natural killer (NK) cells, high levels of interleukin (IL)-1, and a good response to treatments that block IL-1. Osteo-articular (OA) involvement is a key clinical feature of SAPHO. It affects the anterior chest wall, axial skeleton, peripheral joints, mandible, long bones of the extremities, and pelvis. Dermatological involvement is a common target in SAPHO, with lesions observed in 60-90% of cases. Common skin lesions include psoriasis and acne, with hidradenitis suppurativa and neutrophilic dermatoses being less commonly seen. Other clinical findings include constitutional symptoms caused by systemic inflammation, such as fever, weight loss, and fatigue. There is no specific laboratory finding for SAPHO syndrome. However, during active disease, there may be an increase in positive acute phase markers, such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), complement levels, mild leukocytosis, and thrombocytosis. Diagnosis is crucial for SAPHO syndrome, which lacks a specific diagnostic finding and is often underrecognized. A comprehensive evaluation of a patient's medical history and physical examination is crucial. Treatment options include non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, conventional and synthetic disease-modifying agents (cDMARDs and sDMARDs), biological therapies, bisphosphonates, and antibiotics. Biological treatments have emerged as a viable alternative for SAPHO patients who do not respond to conventional treatments.
期刊介绍:
RHEUMATOLOGY INTERNATIONAL is an independent journal reflecting world-wide progress in the research, diagnosis and treatment of the various rheumatic diseases. It is designed to serve researchers and clinicians in the field of rheumatology.
RHEUMATOLOGY INTERNATIONAL will cover all modern trends in clinical research as well as in the management of rheumatic diseases. Special emphasis will be given to public health issues related to rheumatic diseases, applying rheumatology research to clinical practice, epidemiology of rheumatic diseases, diagnostic tests for rheumatic diseases, patient reported outcomes (PROs) in rheumatology and evidence on education of rheumatology. Contributions to these topics will appear in the form of original publications, short communications, editorials, and reviews. "Letters to the editor" will be welcome as an enhancement to discussion. Basic science research, including in vitro or animal studies, is discouraged to submit, as we will only review studies on humans with an epidemological or clinical perspective. Case reports without a proper review of the literatura (Case-based Reviews) will not be published. Every effort will be made to ensure speed of publication while maintaining a high standard of contents and production.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1964 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


