{"title":"赞比亚住院儿童造影剂相关性急性肾损伤的负担和危险因素:大学教学医院的前瞻性队列研究。","authors":"Hellen M'hango, Chishiba Kabengele, Veronica Sukuntu, Chisambo Mwaba","doi":"10.1177/20543581231205156","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Contrast-associated acute kidney injury (CAAKI) is defined as acute kidney injury (AKI) occurring within 72 hours of administration of contrast media (CM) and is linked to adverse outcomes including longer hospital stay, increased hospital mortality, and a higher risk of chronic kidney disease in later life. Risk factors for the development of CAAKI in the Zambian pediatric population have not been well studied.</p><p><strong>Objectives: </strong>The objective of this study was to assess the burden of CAAKI, ascertain its risk factors, and describe short-term outcomes in hospitalized children at the University Teaching Hospitals (UTH) undergoing contrast-enhanced radiological investigations.</p><p><strong>Methods: </strong>This was a prospective observational study of in-patients undergoing contrast-enhanced radiological procedures, between September 2020 and September 2021. The participants were recruited from the Children's Hospital, the Cancer Diseases Hospital, and the Pediatric Surgical Ward at the University Teaching Hospital in Lusaka, Zambia. The primary outcome variable was occurrence of AKI at 48 hours post CM administration. We used 2 criteria to define CAAKI in our study-the European Society of Urogenital Radiology (ESUR) and the Kidney Disease Improving Global Outcomes (KDIGO) 2012 criteria. Multivariable logistic regression models were formulated to assess for risk factors of CAAKI.</p><p><strong>Results: </strong>Of the 201 enrolled participants, 123 (61.2%) were male and the median age of the participants was 5 years (interquartile range [IQR] = 3-10). The mean hemoglobin was 103 g/L (standard deviation [SD] = 26), median creatinine was 30.9 µmol/l (IQR = 22.6-43), and the glomerular filtration rate (GFR) was 102.5 mL/min/1.73 m<sup>2</sup> (IQR = 76.2-129.4). Forty-six (22.9%) developed CAAKI using the ESUR compared with 4.5% (9/201) using the KDIGO criteria. Independent risk factors of CAAKI were receiving a higher dose of CM (adjusted odds ratio [aOR] = 2.54; 95% confidence interval [CI] = [1.12-5.74]), prematurity (aOR = 4.6; 95% CI = [1.05-16.7]), and a higher eGFR (aOR= 1.01; 95% CI = [1.01-1.02]). Females had higher odds of CAAKI (aOR = 2.48; 95% CI = [1.18-5.18]) when compared with males. One CAAKI participant (2.2%) died; none of the participants who developed CAAKI and survived required dialysis and most of them (90%) were discharged before day 7. Day 7 eGFR results had returned to or near baseline values for those whose creatinine results were available.</p><p><strong>Conclusions: </strong>Using the ESUR criteria, a significant proportion (22.9%) of children undergoing contrast-enhanced computed tomography (CT) scans at the UTH developed CAAKI. In contrast, using the KDIGO criteria only 4.5% had CAAKI. Being born as a preterm baby, being female, having a higher eGFR at baseline, and receiving a higher dose of CM were found to be independent risk factors for CAAKI development in Zambian children. Most of the cases of CAAKI in children were transient and of little clinical significance as only a minority of patients developing CAAKI required kidney replacement therapy and all resolved by day 7 post administration of CM.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"10 ","pages":"20543581231205156"},"PeriodicalIF":1.6000,"publicationDate":"2023-10-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fb/b6/10.1177_20543581231205156.PMC10599111.pdf","citationCount":"0","resultStr":"{\"title\":\"Burden and Risk Factors of Contrast-Associated Acute Kidney Injury in Hospitalized Zambian Children: A Prospective Cohort Study at the University Teaching Hospitals.\",\"authors\":\"Hellen M'hango, Chishiba Kabengele, Veronica Sukuntu, Chisambo Mwaba\",\"doi\":\"10.1177/20543581231205156\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Contrast-associated acute kidney injury (CAAKI) is defined as acute kidney injury (AKI) occurring within 72 hours of administration of contrast media (CM) and is linked to adverse outcomes including longer hospital stay, increased hospital mortality, and a higher risk of chronic kidney disease in later life. Risk factors for the development of CAAKI in the Zambian pediatric population have not been well studied.</p><p><strong>Objectives: </strong>The objective of this study was to assess the burden of CAAKI, ascertain its risk factors, and describe short-term outcomes in hospitalized children at the University Teaching Hospitals (UTH) undergoing contrast-enhanced radiological investigations.</p><p><strong>Methods: </strong>This was a prospective observational study of in-patients undergoing contrast-enhanced radiological procedures, between September 2020 and September 2021. The participants were recruited from the Children's Hospital, the Cancer Diseases Hospital, and the Pediatric Surgical Ward at the University Teaching Hospital in Lusaka, Zambia. The primary outcome variable was occurrence of AKI at 48 hours post CM administration. We used 2 criteria to define CAAKI in our study-the European Society of Urogenital Radiology (ESUR) and the Kidney Disease Improving Global Outcomes (KDIGO) 2012 criteria. Multivariable logistic regression models were formulated to assess for risk factors of CAAKI.</p><p><strong>Results: </strong>Of the 201 enrolled participants, 123 (61.2%) were male and the median age of the participants was 5 years (interquartile range [IQR] = 3-10). The mean hemoglobin was 103 g/L (standard deviation [SD] = 26), median creatinine was 30.9 µmol/l (IQR = 22.6-43), and the glomerular filtration rate (GFR) was 102.5 mL/min/1.73 m<sup>2</sup> (IQR = 76.2-129.4). Forty-six (22.9%) developed CAAKI using the ESUR compared with 4.5% (9/201) using the KDIGO criteria. Independent risk factors of CAAKI were receiving a higher dose of CM (adjusted odds ratio [aOR] = 2.54; 95% confidence interval [CI] = [1.12-5.74]), prematurity (aOR = 4.6; 95% CI = [1.05-16.7]), and a higher eGFR (aOR= 1.01; 95% CI = [1.01-1.02]). Females had higher odds of CAAKI (aOR = 2.48; 95% CI = [1.18-5.18]) when compared with males. One CAAKI participant (2.2%) died; none of the participants who developed CAAKI and survived required dialysis and most of them (90%) were discharged before day 7. Day 7 eGFR results had returned to or near baseline values for those whose creatinine results were available.</p><p><strong>Conclusions: </strong>Using the ESUR criteria, a significant proportion (22.9%) of children undergoing contrast-enhanced computed tomography (CT) scans at the UTH developed CAAKI. In contrast, using the KDIGO criteria only 4.5% had CAAKI. Being born as a preterm baby, being female, having a higher eGFR at baseline, and receiving a higher dose of CM were found to be independent risk factors for CAAKI development in Zambian children. Most of the cases of CAAKI in children were transient and of little clinical significance as only a minority of patients developing CAAKI required kidney replacement therapy and all resolved by day 7 post administration of CM.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"10 \",\"pages\":\"20543581231205156\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2023-10-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fb/b6/10.1177_20543581231205156.PMC10599111.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581231205156\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581231205156","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Burden and Risk Factors of Contrast-Associated Acute Kidney Injury in Hospitalized Zambian Children: A Prospective Cohort Study at the University Teaching Hospitals.
Background: Contrast-associated acute kidney injury (CAAKI) is defined as acute kidney injury (AKI) occurring within 72 hours of administration of contrast media (CM) and is linked to adverse outcomes including longer hospital stay, increased hospital mortality, and a higher risk of chronic kidney disease in later life. Risk factors for the development of CAAKI in the Zambian pediatric population have not been well studied.
Objectives: The objective of this study was to assess the burden of CAAKI, ascertain its risk factors, and describe short-term outcomes in hospitalized children at the University Teaching Hospitals (UTH) undergoing contrast-enhanced radiological investigations.
Methods: This was a prospective observational study of in-patients undergoing contrast-enhanced radiological procedures, between September 2020 and September 2021. The participants were recruited from the Children's Hospital, the Cancer Diseases Hospital, and the Pediatric Surgical Ward at the University Teaching Hospital in Lusaka, Zambia. The primary outcome variable was occurrence of AKI at 48 hours post CM administration. We used 2 criteria to define CAAKI in our study-the European Society of Urogenital Radiology (ESUR) and the Kidney Disease Improving Global Outcomes (KDIGO) 2012 criteria. Multivariable logistic regression models were formulated to assess for risk factors of CAAKI.
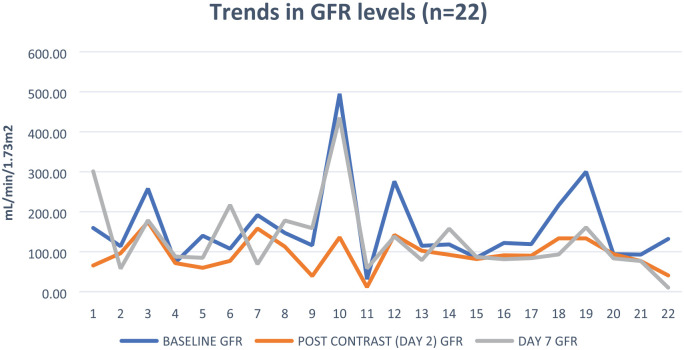
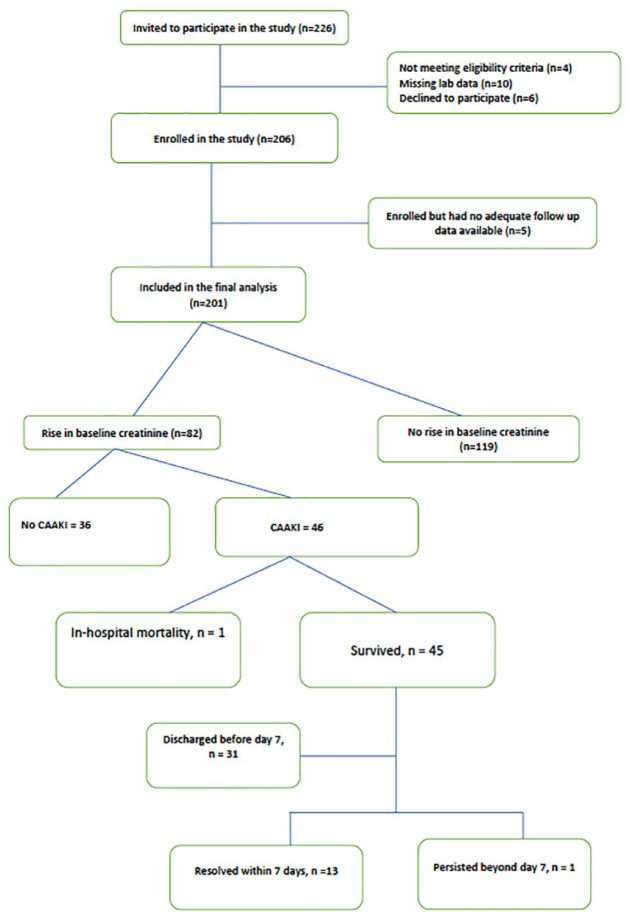
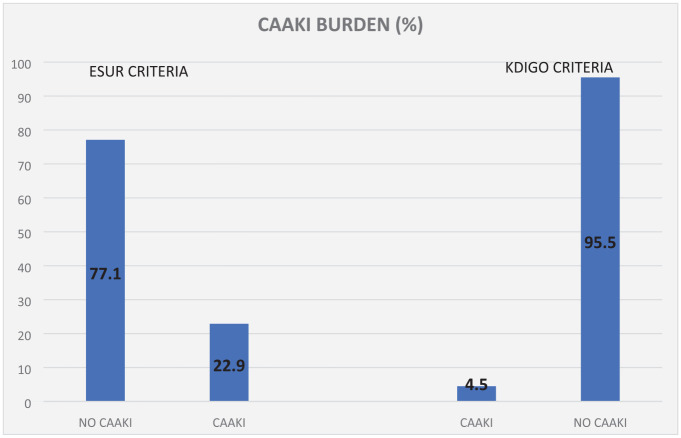
Results: Of the 201 enrolled participants, 123 (61.2%) were male and the median age of the participants was 5 years (interquartile range [IQR] = 3-10). The mean hemoglobin was 103 g/L (standard deviation [SD] = 26), median creatinine was 30.9 µmol/l (IQR = 22.6-43), and the glomerular filtration rate (GFR) was 102.5 mL/min/1.73 m2 (IQR = 76.2-129.4). Forty-six (22.9%) developed CAAKI using the ESUR compared with 4.5% (9/201) using the KDIGO criteria. Independent risk factors of CAAKI were receiving a higher dose of CM (adjusted odds ratio [aOR] = 2.54; 95% confidence interval [CI] = [1.12-5.74]), prematurity (aOR = 4.6; 95% CI = [1.05-16.7]), and a higher eGFR (aOR= 1.01; 95% CI = [1.01-1.02]). Females had higher odds of CAAKI (aOR = 2.48; 95% CI = [1.18-5.18]) when compared with males. One CAAKI participant (2.2%) died; none of the participants who developed CAAKI and survived required dialysis and most of them (90%) were discharged before day 7. Day 7 eGFR results had returned to or near baseline values for those whose creatinine results were available.
Conclusions: Using the ESUR criteria, a significant proportion (22.9%) of children undergoing contrast-enhanced computed tomography (CT) scans at the UTH developed CAAKI. In contrast, using the KDIGO criteria only 4.5% had CAAKI. Being born as a preterm baby, being female, having a higher eGFR at baseline, and receiving a higher dose of CM were found to be independent risk factors for CAAKI development in Zambian children. Most of the cases of CAAKI in children were transient and of little clinical significance as only a minority of patients developing CAAKI required kidney replacement therapy and all resolved by day 7 post administration of CM.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


