Victoria Armstrong, Cynthia Stretch, Liam Fitzgerald, Aquila Gopaul, Greg McKinnon, Jennifer Koziak, Karen Kopciuk, Nigel Brockton, Oliver F. Bathe
{"title":"表征癌症相关的骨骼肌病:低放射密度肌肉的解剖分布和癌症特异性变异性","authors":"Victoria Armstrong, Cynthia Stretch, Liam Fitzgerald, Aquila Gopaul, Greg McKinnon, Jennifer Koziak, Karen Kopciuk, Nigel Brockton, Oliver F. Bathe","doi":"10.1002/rco2.46","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Low muscle radiodensity on computed tomography (CT) scan, indicative of myosteatosis, is commonly observed in cancer patients and can be associated with poor prognosis. Radiodensity is typically measured at the level of the third lumbar vertebra (L3). It is unknown whether features at L3 reflect a systemic state affecting peripheral muscle groups, whether images used at different levels can be used as a surrogate if L3 images are unavailable, and how radiodensity varies between cancer types.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Core and extremity muscle radiodensities were measured in whole body CT images from melanoma patients to evaluate the anatomical distribution of muscle radiodensity measurements. Core muscle radiodensity was measured in 891 patients with different cancer types to study malignancy-dependent patterns in muscle radiodensity.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Low muscle radiodensity at L3 (<30 Hounsfield Unit) was associated with a corresponding lower muscle radiodensity in all muscle groups evaluated (<i>P</i> < 0.001). However, muscle radiodensities were lowest in the core muscle groups compared with muscles in the extremities. Muscle radiodensities at T12 closely correlated with measurements taken at L3 (<i>r</i> = 0.920, <i>P</i> < 0.001), but the correlation was weaker with mid-thigh measurements (<i>r</i> = 0.745, <i>P</i> < 0.001). The distribution of muscle radiodensities varied significantly with cancer type (<i>P</i> = 0.002).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The uniform distribution of low muscle radiodensity in cancer patients supports the hypothesis that the underlying mechanism for myosteatosis is systemic in nature. The most reliable measurements of muscle radiodensity are taken using images of core muscles. Variations in muscle radiodensity associated with cancer exist, suggesting that cancer-specific biological drivers are at play.</p>\n </section>\n </div>","PeriodicalId":73544,"journal":{"name":"JCSM rapid communications","volume":"4 2","pages":"197-206"},"PeriodicalIF":0.0000,"publicationDate":"2021-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/rco2.46","citationCount":"1","resultStr":"{\"title\":\"Characterizing cancer-associated myosteatosis: anatomic distribution and cancer-specific variability of low radiodensity muscle\",\"authors\":\"Victoria Armstrong, Cynthia Stretch, Liam Fitzgerald, Aquila Gopaul, Greg McKinnon, Jennifer Koziak, Karen Kopciuk, Nigel Brockton, Oliver F. Bathe\",\"doi\":\"10.1002/rco2.46\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Low muscle radiodensity on computed tomography (CT) scan, indicative of myosteatosis, is commonly observed in cancer patients and can be associated with poor prognosis. Radiodensity is typically measured at the level of the third lumbar vertebra (L3). It is unknown whether features at L3 reflect a systemic state affecting peripheral muscle groups, whether images used at different levels can be used as a surrogate if L3 images are unavailable, and how radiodensity varies between cancer types.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Core and extremity muscle radiodensities were measured in whole body CT images from melanoma patients to evaluate the anatomical distribution of muscle radiodensity measurements. Core muscle radiodensity was measured in 891 patients with different cancer types to study malignancy-dependent patterns in muscle radiodensity.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Low muscle radiodensity at L3 (<30 Hounsfield Unit) was associated with a corresponding lower muscle radiodensity in all muscle groups evaluated (<i>P</i> < 0.001). However, muscle radiodensities were lowest in the core muscle groups compared with muscles in the extremities. Muscle radiodensities at T12 closely correlated with measurements taken at L3 (<i>r</i> = 0.920, <i>P</i> < 0.001), but the correlation was weaker with mid-thigh measurements (<i>r</i> = 0.745, <i>P</i> < 0.001). The distribution of muscle radiodensities varied significantly with cancer type (<i>P</i> = 0.002).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>The uniform distribution of low muscle radiodensity in cancer patients supports the hypothesis that the underlying mechanism for myosteatosis is systemic in nature. The most reliable measurements of muscle radiodensity are taken using images of core muscles. Variations in muscle radiodensity associated with cancer exist, suggesting that cancer-specific biological drivers are at play.</p>\\n </section>\\n </div>\",\"PeriodicalId\":73544,\"journal\":{\"name\":\"JCSM rapid communications\",\"volume\":\"4 2\",\"pages\":\"197-206\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-06-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/rco2.46\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JCSM rapid communications\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/rco2.46\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCSM rapid communications","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/rco2.46","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
背景计算机断层扫描(CT)显示低肌肉放射密度,表明肌骨化症,在癌症患者中很常见,并可能与不良预后有关。放射密度通常在第三腰椎(L3)水平测量。目前尚不清楚L3的特征是否反映了影响周围肌肉群的系统状态,如果无法获得L3图像,是否可以使用不同级别的图像作为替代,以及不同癌症类型的放射密度如何变化。方法在黑色素瘤患者全身CT图像上测量核心和四肢肌肉放射密度,评价肌肉放射密度的解剖分布。我们测量了891名不同癌症类型患者的核心肌肉放射密度,以研究肌肉放射密度的恶性依赖模式。结果L3 (30 Hounsfield Unit)低肌肉放射密度与所有评估肌肉组相应的低肌肉放射密度相关(P <0.001)。然而,与四肢肌肉相比,核心肌群的肌肉放射密度最低。T12时的肌肉放射密度与L3时的测量值密切相关(r = 0.920, P <0.001),但与大腿中部测量的相关性较弱(r = 0.745, P <0.001)。不同癌症类型的肌肉放射密度分布差异有统计学意义(P = 0.002)。结论肿瘤患者低肌肉放射密度的均匀分布支持了骨化病的潜在机制是全身性的假设。最可靠的肌肉放射密度测量是使用核心肌肉的图像。存在与癌症相关的肌肉放射密度变化,表明癌症特异性生物驱动因素在起作用。
Characterizing cancer-associated myosteatosis: anatomic distribution and cancer-specific variability of low radiodensity muscle
Background
Low muscle radiodensity on computed tomography (CT) scan, indicative of myosteatosis, is commonly observed in cancer patients and can be associated with poor prognosis. Radiodensity is typically measured at the level of the third lumbar vertebra (L3). It is unknown whether features at L3 reflect a systemic state affecting peripheral muscle groups, whether images used at different levels can be used as a surrogate if L3 images are unavailable, and how radiodensity varies between cancer types.
Methods
Core and extremity muscle radiodensities were measured in whole body CT images from melanoma patients to evaluate the anatomical distribution of muscle radiodensity measurements. Core muscle radiodensity was measured in 891 patients with different cancer types to study malignancy-dependent patterns in muscle radiodensity.
Results
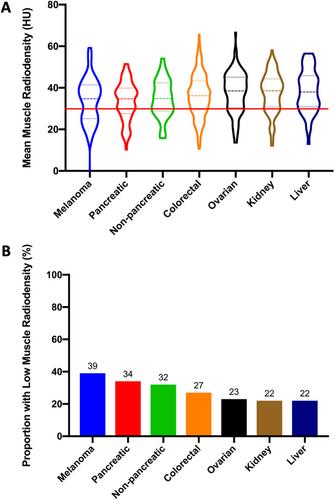
Low muscle radiodensity at L3 (<30 Hounsfield Unit) was associated with a corresponding lower muscle radiodensity in all muscle groups evaluated (P < 0.001). However, muscle radiodensities were lowest in the core muscle groups compared with muscles in the extremities. Muscle radiodensities at T12 closely correlated with measurements taken at L3 (r = 0.920, P < 0.001), but the correlation was weaker with mid-thigh measurements (r = 0.745, P < 0.001). The distribution of muscle radiodensities varied significantly with cancer type (P = 0.002).
Conclusions
The uniform distribution of low muscle radiodensity in cancer patients supports the hypothesis that the underlying mechanism for myosteatosis is systemic in nature. The most reliable measurements of muscle radiodensity are taken using images of core muscles. Variations in muscle radiodensity associated with cancer exist, suggesting that cancer-specific biological drivers are at play.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


