Elaine S. Rogers, Rita Sasidharan, Graeme M. Sequeira, Matthew R. Wood, Stephen P. Bird, Justin W.L. Keogh, Bruce Arroll, Joanna Stewart, Roderick D. MacLeod
{"title":"癌症恶病质的多靶点治疗方法:奥克兰癌症恶病质评估抵抗训练(ACCeRT)试验","authors":"Elaine S. Rogers, Rita Sasidharan, Graeme M. Sequeira, Matthew R. Wood, Stephen P. Bird, Justin W.L. Keogh, Bruce Arroll, Joanna Stewart, Roderick D. MacLeod","doi":"10.1002/rco2.10","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Cancer cachexia is a condition often seen at diagnosis, throughout anti-cancer treatments and in end-stage non-small-cell lung cancer patients.</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>Participants with late-stage non-small-cell lung cancer and cachexia (defined as ≥5% weight loss within 12 months) were randomly assigned 1:2 to 2.09 g of eicosapentaenoic acid (EPA) and 300 mg of cyclo-oxygenase-2 inhibitor celecoxib orally once daily vs. same dosing of EPA, celecoxib, plus two sessions per week of progressive resistance training and 20 g of oral essential amino acids high in leucine in a split dose over 3 days, after each session. Primary endpoint was the acceptability of the earlier multi-targeted approach. Main secondary endpoints included change in body weight and fat-free mass, by bioelectric impedance analysis and total quadriceps muscle volume by magnetic resonance imaging over 20 weeks. Sixty-nine patients were screened resulting in 20 patients being enrolled. Acceptability scored high, with 4.5/5 (Arm A) and 5/5 (Arm B) for EPA and 5/5 for celecoxib within both arms and 4.8/5 for progressive resistance training sessions and 4.5/5 for essential amino acids within Arm B, all at Week 20. Results showed a net gain in bioelectric impedance analysis fat-free mass of +1.3 kg, n = 2 (Arm A), compared with +0.7 kg, n = 7 (Arm B) at Week 12, and —1.5 kg, n = 2 (Arm A), compared with —1.7 kg, n = 4 (Arm B) at Week 20. Trends in efficacy in terms of improvement and/or stability in cachexia markers were seen within magnetic resonance imaging muscle volume, albumin, and C-reactive protein levels within both arms. There were no exercise-related adverse events, with one possible related adverse event of asymptomatic atrial fibrillation in one participant within Arm A.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Non-small-cell lung cancer cachectic patients are willing to be enrolled onto a multi-targeted treatment regimen and may benefit from cachexia symptom management even during the late/refractory stage.</p>\n </section>\n </div>","PeriodicalId":73544,"journal":{"name":"JCSM rapid communications","volume":"3 1","pages":"11-24"},"PeriodicalIF":0.0000,"publicationDate":"2020-02-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/rco2.10","citationCount":"3","resultStr":"{\"title\":\"A multi-targeted treatment approach to cancer cachexia: Auckland's Cancer Cachexia evaluating Resistance Training (ACCeRT) trial\",\"authors\":\"Elaine S. Rogers, Rita Sasidharan, Graeme M. Sequeira, Matthew R. Wood, Stephen P. Bird, Justin W.L. Keogh, Bruce Arroll, Joanna Stewart, Roderick D. MacLeod\",\"doi\":\"10.1002/rco2.10\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Cancer cachexia is a condition often seen at diagnosis, throughout anti-cancer treatments and in end-stage non-small-cell lung cancer patients.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>Participants with late-stage non-small-cell lung cancer and cachexia (defined as ≥5% weight loss within 12 months) were randomly assigned 1:2 to 2.09 g of eicosapentaenoic acid (EPA) and 300 mg of cyclo-oxygenase-2 inhibitor celecoxib orally once daily vs. same dosing of EPA, celecoxib, plus two sessions per week of progressive resistance training and 20 g of oral essential amino acids high in leucine in a split dose over 3 days, after each session. Primary endpoint was the acceptability of the earlier multi-targeted approach. Main secondary endpoints included change in body weight and fat-free mass, by bioelectric impedance analysis and total quadriceps muscle volume by magnetic resonance imaging over 20 weeks. Sixty-nine patients were screened resulting in 20 patients being enrolled. Acceptability scored high, with 4.5/5 (Arm A) and 5/5 (Arm B) for EPA and 5/5 for celecoxib within both arms and 4.8/5 for progressive resistance training sessions and 4.5/5 for essential amino acids within Arm B, all at Week 20. Results showed a net gain in bioelectric impedance analysis fat-free mass of +1.3 kg, n = 2 (Arm A), compared with +0.7 kg, n = 7 (Arm B) at Week 12, and —1.5 kg, n = 2 (Arm A), compared with —1.7 kg, n = 4 (Arm B) at Week 20. Trends in efficacy in terms of improvement and/or stability in cachexia markers were seen within magnetic resonance imaging muscle volume, albumin, and C-reactive protein levels within both arms. There were no exercise-related adverse events, with one possible related adverse event of asymptomatic atrial fibrillation in one participant within Arm A.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Non-small-cell lung cancer cachectic patients are willing to be enrolled onto a multi-targeted treatment regimen and may benefit from cachexia symptom management even during the late/refractory stage.</p>\\n </section>\\n </div>\",\"PeriodicalId\":73544,\"journal\":{\"name\":\"JCSM rapid communications\",\"volume\":\"3 1\",\"pages\":\"11-24\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-02-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/rco2.10\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JCSM rapid communications\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/rco2.10\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCSM rapid communications","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/rco2.10","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
摘要
癌症恶病质是一种常见于诊断、抗癌治疗和终末期非小细胞肺癌患者的疾病。方法和结果晚期非小细胞肺癌和恶恶质(定义为12个月内体重减轻≥5%)的参与者随机分配为1:2至2.09 g二十碳五烯酸(EPA)和300 mg环氧合酶-2抑制剂塞来昔布,每日口服一次,与相同剂量的EPA,塞来昔布加每周两次的渐进式阻力训练和20 g口服高赖氨酸必需氨基酸,分次服用3天。每次会议结束后。主要终点是早期多靶点治疗方法的可接受性。主要次要终点包括体重和无脂质量的变化,通过生物电阻抗分析和磁共振成像的总股四头肌体积在20周内。69名患者被筛选,20名患者入选。在第20周,EPA的可接受性得分很高,在两个组中,塞来昔布的可接受性分别为4.5/5 (A组)和5/5 (B组),渐进阻力训练的可接受性为4.8/5,B组中必需氨基酸的可接受性为4.5/5。结果显示,在生物电阻抗分析中,净增加的无脂质量为+1.3 kg, n = 2 (a组),而在第12周时为+0.7 kg, n = 7 (B组),在第20周时为-1.5 kg, n = 2 (a组),而在第20周时为-1.7 kg, n = 4 (B组)。在磁共振成像肌肉体积、白蛋白和c反应蛋白水平中,可以看到恶病质标志物改善和/或稳定性方面的疗效趋势。没有运动相关的不良事件,在a组中有一名参与者可能出现无症状房颤的不良事件。结论非小细胞肺癌恶病质患者愿意参加多靶向治疗方案,即使在晚期/难治期也可能从恶病质症状管理中获益。
A multi-targeted treatment approach to cancer cachexia: Auckland's Cancer Cachexia evaluating Resistance Training (ACCeRT) trial
Background
Cancer cachexia is a condition often seen at diagnosis, throughout anti-cancer treatments and in end-stage non-small-cell lung cancer patients.
Methods and results
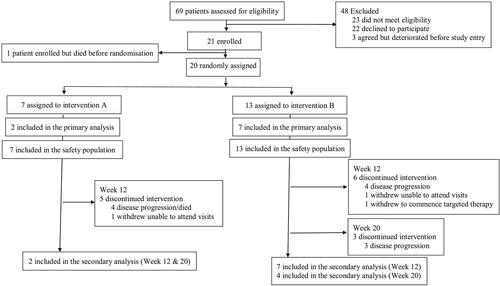
Participants with late-stage non-small-cell lung cancer and cachexia (defined as ≥5% weight loss within 12 months) were randomly assigned 1:2 to 2.09 g of eicosapentaenoic acid (EPA) and 300 mg of cyclo-oxygenase-2 inhibitor celecoxib orally once daily vs. same dosing of EPA, celecoxib, plus two sessions per week of progressive resistance training and 20 g of oral essential amino acids high in leucine in a split dose over 3 days, after each session. Primary endpoint was the acceptability of the earlier multi-targeted approach. Main secondary endpoints included change in body weight and fat-free mass, by bioelectric impedance analysis and total quadriceps muscle volume by magnetic resonance imaging over 20 weeks. Sixty-nine patients were screened resulting in 20 patients being enrolled. Acceptability scored high, with 4.5/5 (Arm A) and 5/5 (Arm B) for EPA and 5/5 for celecoxib within both arms and 4.8/5 for progressive resistance training sessions and 4.5/5 for essential amino acids within Arm B, all at Week 20. Results showed a net gain in bioelectric impedance analysis fat-free mass of +1.3 kg, n = 2 (Arm A), compared with +0.7 kg, n = 7 (Arm B) at Week 12, and —1.5 kg, n = 2 (Arm A), compared with —1.7 kg, n = 4 (Arm B) at Week 20. Trends in efficacy in terms of improvement and/or stability in cachexia markers were seen within magnetic resonance imaging muscle volume, albumin, and C-reactive protein levels within both arms. There were no exercise-related adverse events, with one possible related adverse event of asymptomatic atrial fibrillation in one participant within Arm A.
Conclusions
Non-small-cell lung cancer cachectic patients are willing to be enrolled onto a multi-targeted treatment regimen and may benefit from cachexia symptom management even during the late/refractory stage.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


