{"title":"胫骨神经刺激治疗多发性硬化症患者神经源性下尿路功能障碍的疗效:系统回顾和荟萃分析。","authors":"Fateme Tahmasbi, Samaneh Hosseini, Sakineh Hajebrahimi, Reza Mosaddeghi Heris, Hanieh Salehi-Pourmehr","doi":"10.5152/tud.2023.22241","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study was performed to systematically review the current literature on the effects of transcutaneous tibial nerve stimulation and percutaneous tibial nerve stimulation on multiple sclerosis-induced neurogenic lower urinary tract dysfunction.</p><p><strong>Materials and methods: </strong>Medical databases including PubMed, Scopus, Embase, and Web of Science were systematically searched from inception to September 2022. Metaanalysis was carried out using the comprehensive meta-analysis tool.</p><p><strong>Results: </strong>Our inclusion criteria were met by 12 studies evaluating the effects of percutaneous tibial nerve stimulation/transcutaneous tibial nerve stimulation on multiple sclerosis-induced neurogenic lower urinary tract dysfunction. Comparing the postintervention results to the baseline showed that the rate of frequency was decreased in both percutaneous tibial nerve stimulation and transcutaneous tibial nerve stimulation groups after intervention. The overall mean change of tibial nerve stimulation on frequency was -2.623 (95% CI: -3.58, -1.66; P < .001, I 2 : 87.04) among 6 eligible studies. The post-void residual was decreased after treatment in both methods of tibial nerve stimulation, with an overall mean difference of -31.13 mL (95% CI: -50.62, -11.63; P=.002, I 2 : 71.81). The other urinary parameters, including urgency (mean difference: -4.69; 95% CI: -7.64, -1.74; P < .001, I 2 : 92.16), maximum cystometric capacity (mean difference: 70.95; 95% CI: 44.69, 97.21; P < .001, I 2 : 89.04), and nocturia (mean difference: -1.41; 95% CI: -2.22, 0.60; P < .001, I 2 : 95.15), were improved after intervention, too. However, the results of subgroup analysis showed no effect of transcutaneous tibial nerve stimulation on urinary incontinence (mean difference: -2.00; 95% CI: -4.06, 0.06; P=.057, I 2 : 95.22) and nocturia (mean difference: -0.39; 95% CI: -1.15, 0.37; P=.315, I 2 : 84.01). In terms of mean voided volume, the evidence was related to only percutaneous tibial nerve stimulation with a mean change of 75.01 mL (95% CI: -39.40, 110.61; P < .001, I 2 : 85.04).</p><p><strong>Conclusion: </strong>Although the current literature suggests that tibial nerve electrostimulation might be an effective method for treating neurogenic lower urinary tract dysfunction, the evidence base is poor and derived from small, mostly nonrandomized trials with a high risk of bias and confounding.</p>","PeriodicalId":101337,"journal":{"name":"Urology research & practice","volume":"49 2","pages":"100-111"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10192727/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy of Tibial Nerve Stimulation in Neurogenic Lower Urinary Tract Dysfunction Among Patients with Multiple Sclerosis: A Systematic Review and Meta-analysis.\",\"authors\":\"Fateme Tahmasbi, Samaneh Hosseini, Sakineh Hajebrahimi, Reza Mosaddeghi Heris, Hanieh Salehi-Pourmehr\",\"doi\":\"10.5152/tud.2023.22241\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study was performed to systematically review the current literature on the effects of transcutaneous tibial nerve stimulation and percutaneous tibial nerve stimulation on multiple sclerosis-induced neurogenic lower urinary tract dysfunction.</p><p><strong>Materials and methods: </strong>Medical databases including PubMed, Scopus, Embase, and Web of Science were systematically searched from inception to September 2022. Metaanalysis was carried out using the comprehensive meta-analysis tool.</p><p><strong>Results: </strong>Our inclusion criteria were met by 12 studies evaluating the effects of percutaneous tibial nerve stimulation/transcutaneous tibial nerve stimulation on multiple sclerosis-induced neurogenic lower urinary tract dysfunction. Comparing the postintervention results to the baseline showed that the rate of frequency was decreased in both percutaneous tibial nerve stimulation and transcutaneous tibial nerve stimulation groups after intervention. The overall mean change of tibial nerve stimulation on frequency was -2.623 (95% CI: -3.58, -1.66; P < .001, I 2 : 87.04) among 6 eligible studies. The post-void residual was decreased after treatment in both methods of tibial nerve stimulation, with an overall mean difference of -31.13 mL (95% CI: -50.62, -11.63; P=.002, I 2 : 71.81). The other urinary parameters, including urgency (mean difference: -4.69; 95% CI: -7.64, -1.74; P < .001, I 2 : 92.16), maximum cystometric capacity (mean difference: 70.95; 95% CI: 44.69, 97.21; P < .001, I 2 : 89.04), and nocturia (mean difference: -1.41; 95% CI: -2.22, 0.60; P < .001, I 2 : 95.15), were improved after intervention, too. However, the results of subgroup analysis showed no effect of transcutaneous tibial nerve stimulation on urinary incontinence (mean difference: -2.00; 95% CI: -4.06, 0.06; P=.057, I 2 : 95.22) and nocturia (mean difference: -0.39; 95% CI: -1.15, 0.37; P=.315, I 2 : 84.01). In terms of mean voided volume, the evidence was related to only percutaneous tibial nerve stimulation with a mean change of 75.01 mL (95% CI: -39.40, 110.61; P < .001, I 2 : 85.04).</p><p><strong>Conclusion: </strong>Although the current literature suggests that tibial nerve electrostimulation might be an effective method for treating neurogenic lower urinary tract dysfunction, the evidence base is poor and derived from small, mostly nonrandomized trials with a high risk of bias and confounding.</p>\",\"PeriodicalId\":101337,\"journal\":{\"name\":\"Urology research & practice\",\"volume\":\"49 2\",\"pages\":\"100-111\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10192727/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Urology research & practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5152/tud.2023.22241\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"0\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology research & practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/tud.2023.22241","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:本研究系统回顾了经皮胫骨神经刺激和经皮胫神经刺激对多发性硬化诱导的神经源性下尿路功能障碍的影响的现有文献。材料和方法:从成立到2022年9月,系统搜索了PubMed、Scopus、Embase和Web of Science等医学数据库。使用综合荟萃分析工具进行荟萃分析。结果:12项研究评估了经皮胫骨神经刺激/经皮胫神经刺激对多发性硬化诱导的神经源性下尿路功能障碍的影响,符合我们的纳入标准。将干预后的结果与基线进行比较显示,干预后经皮胫骨神经刺激组和经皮胫神经刺激组的频率均降低。在6项符合条件的研究中,胫骨神经刺激频率的总体平均变化为-2.623(95%CI:3.58,-1.66;P<.001,I2:87.04)。两种胫神经刺激方法治疗后,排尿后残余量均减少,总体平均差异为-31.13 mL(95%可信区间:-50.62,-11.63;P=0.002,I2:71.81)。其他尿路参数,包括紧迫性(平均差异:-4.69;95%可信区间为-7.64,-1.74;P<.001,I2:92.16),最大膀胱测量能力(平均差异:70.95;95%CI:44.69,97.21;P<.001,I2:89.04)和夜尿(平均差异为-1.41;95%CI:2.22,0.60;P<0.001,I2:95.15)也在干预后得到改善。然而,亚组分析结果显示,经皮胫神经刺激对尿失禁(平均差异:-2.00;95%可信区间:-4.06.0.06;P=0.057,I2:95.22)和夜尿(平均差异为-0.39;95%置信区间:-1.15.037;P=.315,I2:84.01)没有影响,证据仅与经皮胫神经刺激有关,平均变化75.01mL(95%可信区间:-39.40,110.61;P<.001,I2:85.04)。结论:尽管目前的文献表明胫神经电刺激可能是治疗神经源性下尿路功能障碍的有效方法,大多数是具有高偏倚和混淆风险的非随机试验。
Efficacy of Tibial Nerve Stimulation in Neurogenic Lower Urinary Tract Dysfunction Among Patients with Multiple Sclerosis: A Systematic Review and Meta-analysis.
Objective: This study was performed to systematically review the current literature on the effects of transcutaneous tibial nerve stimulation and percutaneous tibial nerve stimulation on multiple sclerosis-induced neurogenic lower urinary tract dysfunction.
Materials and methods: Medical databases including PubMed, Scopus, Embase, and Web of Science were systematically searched from inception to September 2022. Metaanalysis was carried out using the comprehensive meta-analysis tool.
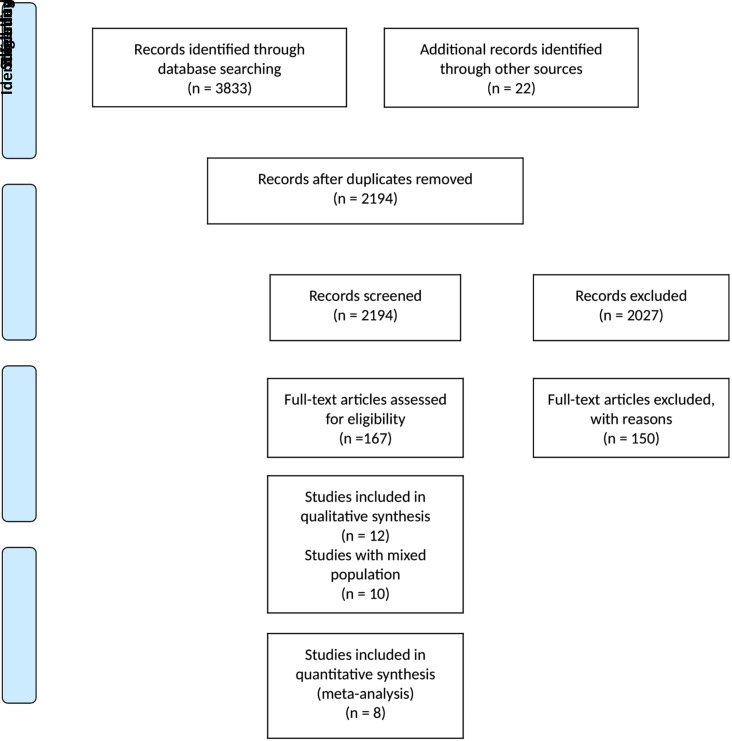
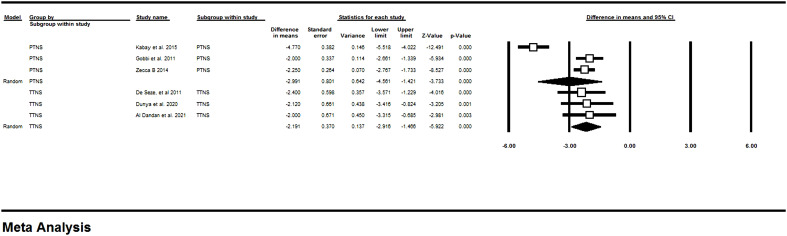
Results: Our inclusion criteria were met by 12 studies evaluating the effects of percutaneous tibial nerve stimulation/transcutaneous tibial nerve stimulation on multiple sclerosis-induced neurogenic lower urinary tract dysfunction. Comparing the postintervention results to the baseline showed that the rate of frequency was decreased in both percutaneous tibial nerve stimulation and transcutaneous tibial nerve stimulation groups after intervention. The overall mean change of tibial nerve stimulation on frequency was -2.623 (95% CI: -3.58, -1.66; P < .001, I 2 : 87.04) among 6 eligible studies. The post-void residual was decreased after treatment in both methods of tibial nerve stimulation, with an overall mean difference of -31.13 mL (95% CI: -50.62, -11.63; P=.002, I 2 : 71.81). The other urinary parameters, including urgency (mean difference: -4.69; 95% CI: -7.64, -1.74; P < .001, I 2 : 92.16), maximum cystometric capacity (mean difference: 70.95; 95% CI: 44.69, 97.21; P < .001, I 2 : 89.04), and nocturia (mean difference: -1.41; 95% CI: -2.22, 0.60; P < .001, I 2 : 95.15), were improved after intervention, too. However, the results of subgroup analysis showed no effect of transcutaneous tibial nerve stimulation on urinary incontinence (mean difference: -2.00; 95% CI: -4.06, 0.06; P=.057, I 2 : 95.22) and nocturia (mean difference: -0.39; 95% CI: -1.15, 0.37; P=.315, I 2 : 84.01). In terms of mean voided volume, the evidence was related to only percutaneous tibial nerve stimulation with a mean change of 75.01 mL (95% CI: -39.40, 110.61; P < .001, I 2 : 85.04).
Conclusion: Although the current literature suggests that tibial nerve electrostimulation might be an effective method for treating neurogenic lower urinary tract dysfunction, the evidence base is poor and derived from small, mostly nonrandomized trials with a high risk of bias and confounding.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


