Ikeoluwapo Kendra Bolakale-Rufai, Shannon M Knapp, Amber E Johnson, LaPrincess Brewer, Selma Mohammed, Daniel Addison, Sula Mazimba, Brownsyne Tucker-Edmonds, Khadijah Breathett
{"title":"种族、心脏病学护理和接受指南指导的围产期心肌病药物治疗之间的关系。","authors":"Ikeoluwapo Kendra Bolakale-Rufai, Shannon M Knapp, Amber E Johnson, LaPrincess Brewer, Selma Mohammed, Daniel Addison, Sula Mazimba, Brownsyne Tucker-Edmonds, Khadijah Breathett","doi":"10.1007/s40615-023-01838-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Black patients with peripartum cardiomyopathy (PPCM) have disproportionately worse outcomes than White patients, possibly related to variable involvement of cardiovascular specialists in their clinical care. We sought to determine whether race was associated with cardiology involvement in clinical care during inpatient admission and whether cardiology involvement in care was associated with higher claims of guideline-directed medical therapy (GDMT) a week after hospital discharge.</p><p><strong>Methods: </strong>Using Optum's de-identified Clinformatics® Data Mart (CDM), we included Black and White patients' first hospital admission for PPCM from 2008 to 2021. Cardiology involvement in clinical care was defined as the receipt of attending care from a cardiovascular specialist during admission. GDMT included beta-blockers (BB) for all patients and triple therapy (BB, angiotensin-responsive medications, and mineralocorticoid receptor antagonists) for non-pregnant patients. Logistic regression was used to determine the associations between cardiology involvement in clinical care during admission and (1) patient race and (2) GDMT prescription, adjusting for age and comorbidities.</p><p><strong>Results: </strong>Among 668 patients (32.6% Black, 67.4% White, 93.3% commercially insured), there was no significant difference in the odds of cardiology involvement in clinical care by race (aOR: 1.41; 95%CI: 0.87-2.33, P=0.17). Inpatient cardiology care was associated with 2.75 times increased odds of having a prescription claim for GDMT (BB) for White patients (aOR: 2.75; 95%CI 1.50-5.06, P=0.001), and the estimated effect size was similar but not statistically significant for Black patients (aOR: 2.20, 95% CI, 0.84-5.71, P=0.11). The interaction between race and cardiology involvement in clinical care was not statistically significant for the receipt of BB prescription. Among 274 non-pregnant patients with PPCM (37.2% Black, 62.8% White), 5.8% received triple GDMT. Of these, none of the Black patients lacking cardiology care had triple GDMT. However, cardiology involvement in care was not significantly associated with triple GDMT for either race.</p><p><strong>Conclusions: </strong>Among a commercially insured population within PPCM, race was not associated with cardiology involvement in clinical care during hospitalization. However, cardiology involvement in care was associated with significantly higher odds of prescription claims for BB for only White patients. Additional strategies are needed to support equitable GDMT prescription.</p>","PeriodicalId":16921,"journal":{"name":"Journal of Racial and Ethnic Health Disparities","volume":" ","pages":"3872-3881"},"PeriodicalIF":3.2000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11035491/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association Between Race, Cardiology Care, and the Receipt of Guideline-Directed Medical Therapy in Peripartum Cardiomyopathy.\",\"authors\":\"Ikeoluwapo Kendra Bolakale-Rufai, Shannon M Knapp, Amber E Johnson, LaPrincess Brewer, Selma Mohammed, Daniel Addison, Sula Mazimba, Brownsyne Tucker-Edmonds, Khadijah Breathett\",\"doi\":\"10.1007/s40615-023-01838-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Black patients with peripartum cardiomyopathy (PPCM) have disproportionately worse outcomes than White patients, possibly related to variable involvement of cardiovascular specialists in their clinical care. We sought to determine whether race was associated with cardiology involvement in clinical care during inpatient admission and whether cardiology involvement in care was associated with higher claims of guideline-directed medical therapy (GDMT) a week after hospital discharge.</p><p><strong>Methods: </strong>Using Optum's de-identified Clinformatics® Data Mart (CDM), we included Black and White patients' first hospital admission for PPCM from 2008 to 2021. Cardiology involvement in clinical care was defined as the receipt of attending care from a cardiovascular specialist during admission. GDMT included beta-blockers (BB) for all patients and triple therapy (BB, angiotensin-responsive medications, and mineralocorticoid receptor antagonists) for non-pregnant patients. Logistic regression was used to determine the associations between cardiology involvement in clinical care during admission and (1) patient race and (2) GDMT prescription, adjusting for age and comorbidities.</p><p><strong>Results: </strong>Among 668 patients (32.6% Black, 67.4% White, 93.3% commercially insured), there was no significant difference in the odds of cardiology involvement in clinical care by race (aOR: 1.41; 95%CI: 0.87-2.33, P=0.17). Inpatient cardiology care was associated with 2.75 times increased odds of having a prescription claim for GDMT (BB) for White patients (aOR: 2.75; 95%CI 1.50-5.06, P=0.001), and the estimated effect size was similar but not statistically significant for Black patients (aOR: 2.20, 95% CI, 0.84-5.71, P=0.11). The interaction between race and cardiology involvement in clinical care was not statistically significant for the receipt of BB prescription. Among 274 non-pregnant patients with PPCM (37.2% Black, 62.8% White), 5.8% received triple GDMT. Of these, none of the Black patients lacking cardiology care had triple GDMT. However, cardiology involvement in care was not significantly associated with triple GDMT for either race.</p><p><strong>Conclusions: </strong>Among a commercially insured population within PPCM, race was not associated with cardiology involvement in clinical care during hospitalization. However, cardiology involvement in care was associated with significantly higher odds of prescription claims for BB for only White patients. Additional strategies are needed to support equitable GDMT prescription.</p>\",\"PeriodicalId\":16921,\"journal\":{\"name\":\"Journal of Racial and Ethnic Health Disparities\",\"volume\":\" \",\"pages\":\"3872-3881\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11035491/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Racial and Ethnic Health Disparities\",\"FirstCategoryId\":\"88\",\"ListUrlMain\":\"https://doi.org/10.1007/s40615-023-01838-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Racial and Ethnic Health Disparities","FirstCategoryId":"88","ListUrlMain":"https://doi.org/10.1007/s40615-023-01838-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/23 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Association Between Race, Cardiology Care, and the Receipt of Guideline-Directed Medical Therapy in Peripartum Cardiomyopathy.
Background: Black patients with peripartum cardiomyopathy (PPCM) have disproportionately worse outcomes than White patients, possibly related to variable involvement of cardiovascular specialists in their clinical care. We sought to determine whether race was associated with cardiology involvement in clinical care during inpatient admission and whether cardiology involvement in care was associated with higher claims of guideline-directed medical therapy (GDMT) a week after hospital discharge.
Methods: Using Optum's de-identified Clinformatics® Data Mart (CDM), we included Black and White patients' first hospital admission for PPCM from 2008 to 2021. Cardiology involvement in clinical care was defined as the receipt of attending care from a cardiovascular specialist during admission. GDMT included beta-blockers (BB) for all patients and triple therapy (BB, angiotensin-responsive medications, and mineralocorticoid receptor antagonists) for non-pregnant patients. Logistic regression was used to determine the associations between cardiology involvement in clinical care during admission and (1) patient race and (2) GDMT prescription, adjusting for age and comorbidities.
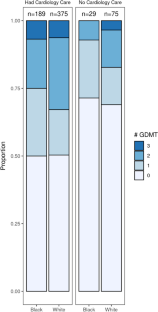
Results: Among 668 patients (32.6% Black, 67.4% White, 93.3% commercially insured), there was no significant difference in the odds of cardiology involvement in clinical care by race (aOR: 1.41; 95%CI: 0.87-2.33, P=0.17). Inpatient cardiology care was associated with 2.75 times increased odds of having a prescription claim for GDMT (BB) for White patients (aOR: 2.75; 95%CI 1.50-5.06, P=0.001), and the estimated effect size was similar but not statistically significant for Black patients (aOR: 2.20, 95% CI, 0.84-5.71, P=0.11). The interaction between race and cardiology involvement in clinical care was not statistically significant for the receipt of BB prescription. Among 274 non-pregnant patients with PPCM (37.2% Black, 62.8% White), 5.8% received triple GDMT. Of these, none of the Black patients lacking cardiology care had triple GDMT. However, cardiology involvement in care was not significantly associated with triple GDMT for either race.
Conclusions: Among a commercially insured population within PPCM, race was not associated with cardiology involvement in clinical care during hospitalization. However, cardiology involvement in care was associated with significantly higher odds of prescription claims for BB for only White patients. Additional strategies are needed to support equitable GDMT prescription.
期刊介绍:
Journal of Racial and Ethnic Health Disparities reports on the scholarly progress of work to understand, address, and ultimately eliminate health disparities based on race and ethnicity. Efforts to explore underlying causes of health disparities and to describe interventions that have been undertaken to address racial and ethnic health disparities are featured. Promising studies that are ongoing or studies that have longer term data are welcome, as are studies that serve as lessons for best practices in eliminating health disparities. Original research, systematic reviews, and commentaries presenting the state-of-the-art thinking on problems centered on health disparities will be considered for publication. We particularly encourage review articles that generate innovative and testable ideas, and constructive discussions and/or critiques of health disparities.Because the Journal of Racial and Ethnic Health Disparities receives a large number of submissions, about 30% of submissions to the Journal are sent out for full peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


