{"title":"免疫工程的黄金时代。","authors":"Wilson W. Wong, Wendell A. Lim","doi":"10.1111/imr.13283","DOIUrl":null,"url":null,"abstract":"<p>Immunology has long been the source of many significant medical breakthroughs, from vaccines for infections to therapeutics for cancer, autoimmunity, and transplant rejection. Indeed, the only diseases we have successfully eradicated, for example, smallpox and polio, were achieved through our understanding of the immune system. Furthermore, the immune system often plays an unexpected role in the outcome of a treatment not designed to engage the immune system. For instance, many chemotherapy or radiation therapies were initially designed to target cancer cells directly. However, subsequent investigations have uncovered the critical role these therapies have in stimulating the immune system.</p><p>As our understanding of the immune system deepens, its involvement in homeostasis and surveillance in almost every human organ becomes more apparent. For instance, the bidirectional response between the immune and central nervous systems has now been recognized as a major determinant for some neurodegenerative (e.g., Parkinson's disease) and psychiatric disorders. Other major chronic diseases, such as heart disease and diabetes, are influenced by the immune system. As such, the study of disease mechanisms would be deemed incomplete without considering the dynamic interaction of the aliment with the immune system. This recognition poses a significant challenge in understanding diseases, especially in humans, because studying the organ of interest is no longer sufficient to get the whole picture.</p><p>Due to its importance, many therapeutics have been developed to modulate the immune response for various diseases. A balance between activation and suppression is critical to maintaining a healthy, functional immune system. For instance, uncontrolled and overactive immune responses can lead to autoimmunity and tissue damage. Yet a hyporesponsive immune system can render the patient vulnerable to infection and cancer development. Many current therapies have been designed to either enhance or restrain the immune system. However, systemic immune system modulation tends to generate severe side effects. Therefore, precise spatiotemporal control of the immune response has become a major focus for the next generation of immunotherapy.</p><p>In this issue, 13 reviews have been prepared by some of the most innovative research groups describing the development of tools and strategies to harness the immune system for therapeutic applications. This issue will not be a comprehensive overview of immunoengineering. Instead, it will focus on applying protein and genetic engineering to improve the safety, specificity, and efficacy of immunotherapies. Furthermore, the immune system's direct interaction with almost all organs provides an intriguing opportunity for innovative and precise medical intervention. The immune system, while highly complex, is also very accessible. One can collect and genetically modify primary human immune cells, essentially converting them into smart drug delivery devices and cell-killing machines with active homing capability that can be remotely controlled by small molecules, light, or ultrasound. These attributes are being explored to treat various immune-mediated diseases (PMID: 37495877).</p><p>Cytokines are small soluble proteins that regulate the immune system and have been exploited as a treatment for many cancer types. The most prominent examples are interleukin- (IL) 2 and interferon-gamma, which are clinically approved. However, due to their ability to widespread inflammation, their toxicity has limited their utility in the clinics. Much effort has been devoted to improving the performance of cytokine therapy, yet success in the clinics has been marginal. Santonelli and Wittrup<span><sup>1</sup></span> elegantly summarize the field and discuss challenges in developing cytokine therapy. They also provide rationales based on engineering principles and clinical data that challenge current conventions and highlight the most promising developments.</p><p>Heller and Spangler's team<span><sup>2</sup></span> dive deeply into the biology of IL-4/IL-13, a specific class of cytokine critical to type 2 inflammatory response. This class is well-known for protecting against multicellular pathogens and is involved in responding to allergens. In addition to providing an overview of the biology, they thoroughly discussed therapeutic and diagnostic opportunities on the IL-4/IL-13 pathway through protein engineering and synthetic gene circuits for allergy, cancer, and other diseases.</p><p>Besides cytokines, other molecules derived from the immune system have enormous biotechnological and therapeutic potential. Antibodies derived from B cells are an example, and we encourage readers to peruse other excellent reviews for the latest developments. Recently, a new class of molecule derived from T-cell receptors (TCR) has emerged as a compelling modality for cancer therapeutics. While less versatile than antibodies, TCR can bind to intracellular-derived peptides, thus accessing mutated intracellular proteins and undruggable targets. Dao, Scheinberg, and their team<span><sup>3</sup></span> discussed the potential and challenge of developing TCR as therapeutics. They also compare TCR to other modalities, such as antibodies and chimeric antigen receptors (CAR). Interestingly, cytokines, antibodies, and TCR can be combined together to create novel therapies (Figure 1).</p><p>Small molecules and biologics are the dominant form of therapeutics. However, advances in cell engineering and synthetic biology have enabled the development of a new modality—immune cell therapy. The most prominent is the chimeric antigen receptor (CAR) T-cell therapy, with six FDA approvals for various hematological malignancies since 2017. Several reviews in this issue cover the foundation of CAR T-cell therapy. Roybal and his team outline some clinical considerations needed to create more effective CAR T-cell therapies.<span><sup>4</sup></span> Maus and colleagues specifically summarize preclinical and clinical results using CAR T cells against various digestive tract cancers and discuss opportunities and hurdles in applying CAR technology to this class of cancer.<span><sup>5</sup></span> Even with this impressive number of approvals in such a short time, these currently approved treatments only represent the foundation for various possibilities.</p><p>The most challenging part of successfully treating cancer has always been killing enough cancer cells while sparing healthy tissues. This typically requires precise delivery or recruitment of cytotoxic agents to the tumor, a challenge that is fundamentally difficult to address with small molecules or antibodies alone. Immune cell therapies are well suited to tackle this challenge, integrating complex genetic circuits into immune cells to enhance their precision. Hernandez-Lopez and his team<span><sup>6</sup></span> have summarized some of the latest developments in genetic circuit design that would improve specificity and provide safety controls to CAR T cells (Figure 2A).</p><p>Designing the optimal receptor is a crucial consideration for ensuring the appropriate function of cellular therapies. An example of where this is of critical importance is the treatment of solid tumors, which have many means of suppressing or evading the immune response. Furthermore, CAR T cells can also suffer from exhaustion through chronic stimulation by the cancer cells. Multiple strategies are available to address these issues related to CAR T potency, with one way being to engineer the CAR to promote survival. Wang, Xu, and their team recently discovered the importance of the electrostatic interaction of the intracellular signaling domain on CARs. Their review<span><sup>7</sup></span> in this issue discusses recent findings and strategies to harness the knowledge of charge-based interaction for designing better CARs (Figure 2A).</p><p>A CAR is comprised of several signaling domains that can impact T-cell physiology in different ways. Comprehensively exploring all the possible combinations of signaling domains in a CAR would be too time-consuming. While incorporating literature data can reduce the CAR design space, a more efficient receptor design approach is needed. Daniels and Capponi<span><sup>8</sup></span> discuss the potential of using artificial intelligence (AI) and machine learning (ML) to improve adoptive immune cell therapy. Specifically, they provide an overview of their recent work constructing a library of CARs and using AI to facilitate and understand the CAR designs that would improve persistence and survival. AI and large-scale cell engineering technology will undoubtedly be one of the primary sources of innovative CAR immune cell therapy design (Figure 2A).</p><p>Besides the receptor, engineering the cell host can improve its performance against cancer cells. Irving and colleagues summarize the concept of “coengineering”,<span><sup>9</sup></span> highlighting the benefit of introducing multiple features besides the tumor-targeting receptor into immune cells to enhance their safety, specificity, and efficacy (Figure 2B). For instance, therapeutic antibodies (e.g., checkpoint inhibitors) or cytokines can be inducibly overexpressed in CAR T cells to enhance their proliferation and survival within the tumor microenvironment. In addition to gene overexpression, directly modifying the genome is an important coengineering approach. CRISPR/Cas has become the most essential tool in genome engineering. Chen and colleagues<span><sup>10</sup></span> summarize the latest developments and experimental considerations in using CRISPR/Cas for unbiased functional screens in immune cells. They also discussed critical advances in creating more potent therapeutic immune cell therapies using CRISPR (Figure 2B). The ever-expanding capability of CRISPR technology will profoundly impact the understanding and development of immunotherapy.</p><p>T cells are the primary cell type for creating CAR immune cell therapy. While T cells have proven to be a potent vehicle for CAR therapy, they also have shortcomings. One of the main challenges in using T cells is that they have a TCR, which leads to graft vs. host disease if the T cells are allogeneically sourced. As such, all clinically approved CAR T-cell therapies use T cells from the patient as the cell source. This drastically increases the complexity and cost of the manufacturing process. It is widely recognized that the next generation of immune cell therapy should be allogeneic or in situ engineered to ensure comprehensive patient access and commercial viability.</p><p>Deleting the TCR from the T-cell genome is one of the most prominent approaches to creating allogeneic CAR T cells. While intriguing, this approach also increases the manufacturing complexity. Therefore, other immune cell types with cell-killing capability that do not express a TCR are also being explored as potential vehicles for CAR. Natural killer (NK) cells are an intriguing alternative to T cells as the cell host because they have proven to be an essential player against cancer. Interestingly, the foundational CAR design also works in NK cells. In the review by Rezvani and colleagues,<span><sup>11</sup></span> they highlight advances and understanding in CAR T and NK cells. Recent clinical trials with CAR NK cells have demonstrated exciting clinical efficacy with fewer side effects than CAR T cells. However, NK cells inherently have a shorter lifespan than T cells. Further advances in improving NK cell activity could pave the way for an off-the-shelf, allogeneic CAR immune cell therapy with activity comparable to T cells but with fewer side effects (Figure 3A).</p><p>In addition to T and NK cells, macrophages are also under investigation as a medium for immune cell therapy. Macrophages can naturally migrate into and accumulate in solid tumors, and many macrophages are routinely observed for various tumors. A modified CAR expressed in macrophages can induce antigen-dependent phagocytosis (Figure 3A). These properties make macrophages an attractive cell host for CAR. Our understanding of macrophage biology in the context of CAR is less than T cells. Gill and colleagues<span><sup>12</sup></span> have prepared a review summarizing the opportunities and challenges of developing CAR macrophages as cancer immunotherapy. Due to their natural abundance and tumor-homing capability over other immune cell types, unlocking the potential of macrophages could have a significant manufacturing advantage.</p><p>Most applications of immune cell therapy are designed for treating cancer. However, engineered immune cells can also be leveraged to tackle autoimmunity and transplant rejection. Autoimmunity and transplant rejection are typically caused by immune cells, such as B and T cells, attacking the patient's healthy tissues or allografts. Only a small subset of B and T cells are auto- or alloreactive. Systemic immunosuppression is the current standard of care, but it is also accompanied by many complications and reduced capacity for the patient to fight infections. Using a CAR approach, CAR T cells have been designed to specifically eradicate only the autoreactive or alloreactive immune cells while sparing other healthy immune cells, thus providing a highly precise approach to address these unwanted immune responses without systemic immunosuppression. However, identifying the autoreactive and alloreactive B and T cells in autoimmune or transplant cases remains challenging. An alternative approach is to leverage regulatory T (Treg) cells, a subset of CD4 T cells that can suppress the immune response when the TCR signaling pathway is activated (Figure 3B). Unsurprisingly, CAR-expressing Treg can lead to antigen-dependent immune suppression. Levings and colleagues<span><sup>13</sup></span> provide a detailed review of designer Treg's past achievements and current status. They also highlight the clinical potential of engineered Treg and discuss the ongoing preclinical studies and clinical trials on using designer Treg for various immune-mediated diseases.</p><p>We are now in the golden age of immunoengineering. The exciting and innovative immunoengineering developments summarized in this special issue of Immunological Reviews illustrate the immense potential that precise control over the immune system could have on developing disease-modifying, maybe even curative, therapies against some of the most untreatable diseases. These developments are, in part, accelerated by the convergence of multiple fields with immunology. For instance, the RNA technology that powers the unprecedented development of COVID vaccines is now being explored to create CAR T cells in situ, thus completely circumventing the need for cumbersome ex vivo cell processing. The main approach being investigated is to encapsulate messenger RNA (mRNA) encoding the gene of interest (e.g., CAR) into lipid nanoparticles and deliver the mRNA to immune cells inside the patient. The mRNA/LNP-based approach was recently leveraged to create CAR T cells against cardiac fibrotic tissues in mice to treat heart disease (PMID: 34990237).</p><p>Most conventional therapies aim to regulate one pathway or one cell type. However, that is different from how the therapy works in the complex, multicellular environment of a patient. For example, we learned from CAR T-cell therapy that we need both CD4 and CD8 T cells to be effective against cancer. Various combination therapies utilizing checkpoint inhibitors engage different parts of the immune response to elicit an efficacious response. Therefore, we anticipate that a purposeful modulation of multiple aspects of the immune system would further unlock the potential of immunotherapy. In addition, the immune response is a dynamic and carefully orchestrated process. We have seen that treating patients with chemotherapy to eliminate specific immune cells before administering CAR T cells could enhance their persistence and anti-cancer efficacy. Thus, considering the temporal order of multi-pronged regulation of the immune system could be the new dimension that can further accelerate the progress of immunotherapy.</p><p>W.W.W. holds equity in Senti Biosciences and 4Immune Therapeutics. W.A.L. holds equity in Gilead Sciences and Intellia Therapeutics and is an adviser for Allogene Therapeutics.</p>","PeriodicalId":178,"journal":{"name":"Immunological Reviews","volume":"320 1","pages":"4-9"},"PeriodicalIF":7.5000,"publicationDate":"2023-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/imr.13283","citationCount":"0","resultStr":"{\"title\":\"Golden age of immunoengineering\",\"authors\":\"Wilson W. Wong, Wendell A. Lim\",\"doi\":\"10.1111/imr.13283\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Immunology has long been the source of many significant medical breakthroughs, from vaccines for infections to therapeutics for cancer, autoimmunity, and transplant rejection. Indeed, the only diseases we have successfully eradicated, for example, smallpox and polio, were achieved through our understanding of the immune system. Furthermore, the immune system often plays an unexpected role in the outcome of a treatment not designed to engage the immune system. For instance, many chemotherapy or radiation therapies were initially designed to target cancer cells directly. However, subsequent investigations have uncovered the critical role these therapies have in stimulating the immune system.</p><p>As our understanding of the immune system deepens, its involvement in homeostasis and surveillance in almost every human organ becomes more apparent. For instance, the bidirectional response between the immune and central nervous systems has now been recognized as a major determinant for some neurodegenerative (e.g., Parkinson's disease) and psychiatric disorders. Other major chronic diseases, such as heart disease and diabetes, are influenced by the immune system. As such, the study of disease mechanisms would be deemed incomplete without considering the dynamic interaction of the aliment with the immune system. This recognition poses a significant challenge in understanding diseases, especially in humans, because studying the organ of interest is no longer sufficient to get the whole picture.</p><p>Due to its importance, many therapeutics have been developed to modulate the immune response for various diseases. A balance between activation and suppression is critical to maintaining a healthy, functional immune system. For instance, uncontrolled and overactive immune responses can lead to autoimmunity and tissue damage. Yet a hyporesponsive immune system can render the patient vulnerable to infection and cancer development. Many current therapies have been designed to either enhance or restrain the immune system. However, systemic immune system modulation tends to generate severe side effects. Therefore, precise spatiotemporal control of the immune response has become a major focus for the next generation of immunotherapy.</p><p>In this issue, 13 reviews have been prepared by some of the most innovative research groups describing the development of tools and strategies to harness the immune system for therapeutic applications. This issue will not be a comprehensive overview of immunoengineering. Instead, it will focus on applying protein and genetic engineering to improve the safety, specificity, and efficacy of immunotherapies. Furthermore, the immune system's direct interaction with almost all organs provides an intriguing opportunity for innovative and precise medical intervention. The immune system, while highly complex, is also very accessible. One can collect and genetically modify primary human immune cells, essentially converting them into smart drug delivery devices and cell-killing machines with active homing capability that can be remotely controlled by small molecules, light, or ultrasound. These attributes are being explored to treat various immune-mediated diseases (PMID: 37495877).</p><p>Cytokines are small soluble proteins that regulate the immune system and have been exploited as a treatment for many cancer types. The most prominent examples are interleukin- (IL) 2 and interferon-gamma, which are clinically approved. However, due to their ability to widespread inflammation, their toxicity has limited their utility in the clinics. Much effort has been devoted to improving the performance of cytokine therapy, yet success in the clinics has been marginal. Santonelli and Wittrup<span><sup>1</sup></span> elegantly summarize the field and discuss challenges in developing cytokine therapy. They also provide rationales based on engineering principles and clinical data that challenge current conventions and highlight the most promising developments.</p><p>Heller and Spangler's team<span><sup>2</sup></span> dive deeply into the biology of IL-4/IL-13, a specific class of cytokine critical to type 2 inflammatory response. This class is well-known for protecting against multicellular pathogens and is involved in responding to allergens. In addition to providing an overview of the biology, they thoroughly discussed therapeutic and diagnostic opportunities on the IL-4/IL-13 pathway through protein engineering and synthetic gene circuits for allergy, cancer, and other diseases.</p><p>Besides cytokines, other molecules derived from the immune system have enormous biotechnological and therapeutic potential. Antibodies derived from B cells are an example, and we encourage readers to peruse other excellent reviews for the latest developments. Recently, a new class of molecule derived from T-cell receptors (TCR) has emerged as a compelling modality for cancer therapeutics. While less versatile than antibodies, TCR can bind to intracellular-derived peptides, thus accessing mutated intracellular proteins and undruggable targets. Dao, Scheinberg, and their team<span><sup>3</sup></span> discussed the potential and challenge of developing TCR as therapeutics. They also compare TCR to other modalities, such as antibodies and chimeric antigen receptors (CAR). Interestingly, cytokines, antibodies, and TCR can be combined together to create novel therapies (Figure 1).</p><p>Small molecules and biologics are the dominant form of therapeutics. However, advances in cell engineering and synthetic biology have enabled the development of a new modality—immune cell therapy. The most prominent is the chimeric antigen receptor (CAR) T-cell therapy, with six FDA approvals for various hematological malignancies since 2017. Several reviews in this issue cover the foundation of CAR T-cell therapy. Roybal and his team outline some clinical considerations needed to create more effective CAR T-cell therapies.<span><sup>4</sup></span> Maus and colleagues specifically summarize preclinical and clinical results using CAR T cells against various digestive tract cancers and discuss opportunities and hurdles in applying CAR technology to this class of cancer.<span><sup>5</sup></span> Even with this impressive number of approvals in such a short time, these currently approved treatments only represent the foundation for various possibilities.</p><p>The most challenging part of successfully treating cancer has always been killing enough cancer cells while sparing healthy tissues. This typically requires precise delivery or recruitment of cytotoxic agents to the tumor, a challenge that is fundamentally difficult to address with small molecules or antibodies alone. Immune cell therapies are well suited to tackle this challenge, integrating complex genetic circuits into immune cells to enhance their precision. Hernandez-Lopez and his team<span><sup>6</sup></span> have summarized some of the latest developments in genetic circuit design that would improve specificity and provide safety controls to CAR T cells (Figure 2A).</p><p>Designing the optimal receptor is a crucial consideration for ensuring the appropriate function of cellular therapies. An example of where this is of critical importance is the treatment of solid tumors, which have many means of suppressing or evading the immune response. Furthermore, CAR T cells can also suffer from exhaustion through chronic stimulation by the cancer cells. Multiple strategies are available to address these issues related to CAR T potency, with one way being to engineer the CAR to promote survival. Wang, Xu, and their team recently discovered the importance of the electrostatic interaction of the intracellular signaling domain on CARs. Their review<span><sup>7</sup></span> in this issue discusses recent findings and strategies to harness the knowledge of charge-based interaction for designing better CARs (Figure 2A).</p><p>A CAR is comprised of several signaling domains that can impact T-cell physiology in different ways. Comprehensively exploring all the possible combinations of signaling domains in a CAR would be too time-consuming. While incorporating literature data can reduce the CAR design space, a more efficient receptor design approach is needed. Daniels and Capponi<span><sup>8</sup></span> discuss the potential of using artificial intelligence (AI) and machine learning (ML) to improve adoptive immune cell therapy. Specifically, they provide an overview of their recent work constructing a library of CARs and using AI to facilitate and understand the CAR designs that would improve persistence and survival. AI and large-scale cell engineering technology will undoubtedly be one of the primary sources of innovative CAR immune cell therapy design (Figure 2A).</p><p>Besides the receptor, engineering the cell host can improve its performance against cancer cells. Irving and colleagues summarize the concept of “coengineering”,<span><sup>9</sup></span> highlighting the benefit of introducing multiple features besides the tumor-targeting receptor into immune cells to enhance their safety, specificity, and efficacy (Figure 2B). For instance, therapeutic antibodies (e.g., checkpoint inhibitors) or cytokines can be inducibly overexpressed in CAR T cells to enhance their proliferation and survival within the tumor microenvironment. In addition to gene overexpression, directly modifying the genome is an important coengineering approach. CRISPR/Cas has become the most essential tool in genome engineering. Chen and colleagues<span><sup>10</sup></span> summarize the latest developments and experimental considerations in using CRISPR/Cas for unbiased functional screens in immune cells. They also discussed critical advances in creating more potent therapeutic immune cell therapies using CRISPR (Figure 2B). The ever-expanding capability of CRISPR technology will profoundly impact the understanding and development of immunotherapy.</p><p>T cells are the primary cell type for creating CAR immune cell therapy. While T cells have proven to be a potent vehicle for CAR therapy, they also have shortcomings. One of the main challenges in using T cells is that they have a TCR, which leads to graft vs. host disease if the T cells are allogeneically sourced. As such, all clinically approved CAR T-cell therapies use T cells from the patient as the cell source. This drastically increases the complexity and cost of the manufacturing process. It is widely recognized that the next generation of immune cell therapy should be allogeneic or in situ engineered to ensure comprehensive patient access and commercial viability.</p><p>Deleting the TCR from the T-cell genome is one of the most prominent approaches to creating allogeneic CAR T cells. While intriguing, this approach also increases the manufacturing complexity. Therefore, other immune cell types with cell-killing capability that do not express a TCR are also being explored as potential vehicles for CAR. Natural killer (NK) cells are an intriguing alternative to T cells as the cell host because they have proven to be an essential player against cancer. Interestingly, the foundational CAR design also works in NK cells. In the review by Rezvani and colleagues,<span><sup>11</sup></span> they highlight advances and understanding in CAR T and NK cells. Recent clinical trials with CAR NK cells have demonstrated exciting clinical efficacy with fewer side effects than CAR T cells. However, NK cells inherently have a shorter lifespan than T cells. Further advances in improving NK cell activity could pave the way for an off-the-shelf, allogeneic CAR immune cell therapy with activity comparable to T cells but with fewer side effects (Figure 3A).</p><p>In addition to T and NK cells, macrophages are also under investigation as a medium for immune cell therapy. Macrophages can naturally migrate into and accumulate in solid tumors, and many macrophages are routinely observed for various tumors. A modified CAR expressed in macrophages can induce antigen-dependent phagocytosis (Figure 3A). These properties make macrophages an attractive cell host for CAR. Our understanding of macrophage biology in the context of CAR is less than T cells. Gill and colleagues<span><sup>12</sup></span> have prepared a review summarizing the opportunities and challenges of developing CAR macrophages as cancer immunotherapy. Due to their natural abundance and tumor-homing capability over other immune cell types, unlocking the potential of macrophages could have a significant manufacturing advantage.</p><p>Most applications of immune cell therapy are designed for treating cancer. However, engineered immune cells can also be leveraged to tackle autoimmunity and transplant rejection. Autoimmunity and transplant rejection are typically caused by immune cells, such as B and T cells, attacking the patient's healthy tissues or allografts. Only a small subset of B and T cells are auto- or alloreactive. Systemic immunosuppression is the current standard of care, but it is also accompanied by many complications and reduced capacity for the patient to fight infections. Using a CAR approach, CAR T cells have been designed to specifically eradicate only the autoreactive or alloreactive immune cells while sparing other healthy immune cells, thus providing a highly precise approach to address these unwanted immune responses without systemic immunosuppression. However, identifying the autoreactive and alloreactive B and T cells in autoimmune or transplant cases remains challenging. An alternative approach is to leverage regulatory T (Treg) cells, a subset of CD4 T cells that can suppress the immune response when the TCR signaling pathway is activated (Figure 3B). Unsurprisingly, CAR-expressing Treg can lead to antigen-dependent immune suppression. Levings and colleagues<span><sup>13</sup></span> provide a detailed review of designer Treg's past achievements and current status. They also highlight the clinical potential of engineered Treg and discuss the ongoing preclinical studies and clinical trials on using designer Treg for various immune-mediated diseases.</p><p>We are now in the golden age of immunoengineering. The exciting and innovative immunoengineering developments summarized in this special issue of Immunological Reviews illustrate the immense potential that precise control over the immune system could have on developing disease-modifying, maybe even curative, therapies against some of the most untreatable diseases. These developments are, in part, accelerated by the convergence of multiple fields with immunology. For instance, the RNA technology that powers the unprecedented development of COVID vaccines is now being explored to create CAR T cells in situ, thus completely circumventing the need for cumbersome ex vivo cell processing. The main approach being investigated is to encapsulate messenger RNA (mRNA) encoding the gene of interest (e.g., CAR) into lipid nanoparticles and deliver the mRNA to immune cells inside the patient. The mRNA/LNP-based approach was recently leveraged to create CAR T cells against cardiac fibrotic tissues in mice to treat heart disease (PMID: 34990237).</p><p>Most conventional therapies aim to regulate one pathway or one cell type. However, that is different from how the therapy works in the complex, multicellular environment of a patient. For example, we learned from CAR T-cell therapy that we need both CD4 and CD8 T cells to be effective against cancer. Various combination therapies utilizing checkpoint inhibitors engage different parts of the immune response to elicit an efficacious response. Therefore, we anticipate that a purposeful modulation of multiple aspects of the immune system would further unlock the potential of immunotherapy. In addition, the immune response is a dynamic and carefully orchestrated process. We have seen that treating patients with chemotherapy to eliminate specific immune cells before administering CAR T cells could enhance their persistence and anti-cancer efficacy. Thus, considering the temporal order of multi-pronged regulation of the immune system could be the new dimension that can further accelerate the progress of immunotherapy.</p><p>W.W.W. holds equity in Senti Biosciences and 4Immune Therapeutics. W.A.L. holds equity in Gilead Sciences and Intellia Therapeutics and is an adviser for Allogene Therapeutics.</p>\",\"PeriodicalId\":178,\"journal\":{\"name\":\"Immunological Reviews\",\"volume\":\"320 1\",\"pages\":\"4-9\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2023-10-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/imr.13283\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Immunological Reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/imr.13283\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Immunological Reviews","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/imr.13283","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Immunology has long been the source of many significant medical breakthroughs, from vaccines for infections to therapeutics for cancer, autoimmunity, and transplant rejection. Indeed, the only diseases we have successfully eradicated, for example, smallpox and polio, were achieved through our understanding of the immune system. Furthermore, the immune system often plays an unexpected role in the outcome of a treatment not designed to engage the immune system. For instance, many chemotherapy or radiation therapies were initially designed to target cancer cells directly. However, subsequent investigations have uncovered the critical role these therapies have in stimulating the immune system.
As our understanding of the immune system deepens, its involvement in homeostasis and surveillance in almost every human organ becomes more apparent. For instance, the bidirectional response between the immune and central nervous systems has now been recognized as a major determinant for some neurodegenerative (e.g., Parkinson's disease) and psychiatric disorders. Other major chronic diseases, such as heart disease and diabetes, are influenced by the immune system. As such, the study of disease mechanisms would be deemed incomplete without considering the dynamic interaction of the aliment with the immune system. This recognition poses a significant challenge in understanding diseases, especially in humans, because studying the organ of interest is no longer sufficient to get the whole picture.
Due to its importance, many therapeutics have been developed to modulate the immune response for various diseases. A balance between activation and suppression is critical to maintaining a healthy, functional immune system. For instance, uncontrolled and overactive immune responses can lead to autoimmunity and tissue damage. Yet a hyporesponsive immune system can render the patient vulnerable to infection and cancer development. Many current therapies have been designed to either enhance or restrain the immune system. However, systemic immune system modulation tends to generate severe side effects. Therefore, precise spatiotemporal control of the immune response has become a major focus for the next generation of immunotherapy.
In this issue, 13 reviews have been prepared by some of the most innovative research groups describing the development of tools and strategies to harness the immune system for therapeutic applications. This issue will not be a comprehensive overview of immunoengineering. Instead, it will focus on applying protein and genetic engineering to improve the safety, specificity, and efficacy of immunotherapies. Furthermore, the immune system's direct interaction with almost all organs provides an intriguing opportunity for innovative and precise medical intervention. The immune system, while highly complex, is also very accessible. One can collect and genetically modify primary human immune cells, essentially converting them into smart drug delivery devices and cell-killing machines with active homing capability that can be remotely controlled by small molecules, light, or ultrasound. These attributes are being explored to treat various immune-mediated diseases (PMID: 37495877).
Cytokines are small soluble proteins that regulate the immune system and have been exploited as a treatment for many cancer types. The most prominent examples are interleukin- (IL) 2 and interferon-gamma, which are clinically approved. However, due to their ability to widespread inflammation, their toxicity has limited their utility in the clinics. Much effort has been devoted to improving the performance of cytokine therapy, yet success in the clinics has been marginal. Santonelli and Wittrup1 elegantly summarize the field and discuss challenges in developing cytokine therapy. They also provide rationales based on engineering principles and clinical data that challenge current conventions and highlight the most promising developments.
Heller and Spangler's team2 dive deeply into the biology of IL-4/IL-13, a specific class of cytokine critical to type 2 inflammatory response. This class is well-known for protecting against multicellular pathogens and is involved in responding to allergens. In addition to providing an overview of the biology, they thoroughly discussed therapeutic and diagnostic opportunities on the IL-4/IL-13 pathway through protein engineering and synthetic gene circuits for allergy, cancer, and other diseases.
Besides cytokines, other molecules derived from the immune system have enormous biotechnological and therapeutic potential. Antibodies derived from B cells are an example, and we encourage readers to peruse other excellent reviews for the latest developments. Recently, a new class of molecule derived from T-cell receptors (TCR) has emerged as a compelling modality for cancer therapeutics. While less versatile than antibodies, TCR can bind to intracellular-derived peptides, thus accessing mutated intracellular proteins and undruggable targets. Dao, Scheinberg, and their team3 discussed the potential and challenge of developing TCR as therapeutics. They also compare TCR to other modalities, such as antibodies and chimeric antigen receptors (CAR). Interestingly, cytokines, antibodies, and TCR can be combined together to create novel therapies (Figure 1).
Small molecules and biologics are the dominant form of therapeutics. However, advances in cell engineering and synthetic biology have enabled the development of a new modality—immune cell therapy. The most prominent is the chimeric antigen receptor (CAR) T-cell therapy, with six FDA approvals for various hematological malignancies since 2017. Several reviews in this issue cover the foundation of CAR T-cell therapy. Roybal and his team outline some clinical considerations needed to create more effective CAR T-cell therapies.4 Maus and colleagues specifically summarize preclinical and clinical results using CAR T cells against various digestive tract cancers and discuss opportunities and hurdles in applying CAR technology to this class of cancer.5 Even with this impressive number of approvals in such a short time, these currently approved treatments only represent the foundation for various possibilities.
The most challenging part of successfully treating cancer has always been killing enough cancer cells while sparing healthy tissues. This typically requires precise delivery or recruitment of cytotoxic agents to the tumor, a challenge that is fundamentally difficult to address with small molecules or antibodies alone. Immune cell therapies are well suited to tackle this challenge, integrating complex genetic circuits into immune cells to enhance their precision. Hernandez-Lopez and his team6 have summarized some of the latest developments in genetic circuit design that would improve specificity and provide safety controls to CAR T cells (Figure 2A).
Designing the optimal receptor is a crucial consideration for ensuring the appropriate function of cellular therapies. An example of where this is of critical importance is the treatment of solid tumors, which have many means of suppressing or evading the immune response. Furthermore, CAR T cells can also suffer from exhaustion through chronic stimulation by the cancer cells. Multiple strategies are available to address these issues related to CAR T potency, with one way being to engineer the CAR to promote survival. Wang, Xu, and their team recently discovered the importance of the electrostatic interaction of the intracellular signaling domain on CARs. Their review7 in this issue discusses recent findings and strategies to harness the knowledge of charge-based interaction for designing better CARs (Figure 2A).
A CAR is comprised of several signaling domains that can impact T-cell physiology in different ways. Comprehensively exploring all the possible combinations of signaling domains in a CAR would be too time-consuming. While incorporating literature data can reduce the CAR design space, a more efficient receptor design approach is needed. Daniels and Capponi8 discuss the potential of using artificial intelligence (AI) and machine learning (ML) to improve adoptive immune cell therapy. Specifically, they provide an overview of their recent work constructing a library of CARs and using AI to facilitate and understand the CAR designs that would improve persistence and survival. AI and large-scale cell engineering technology will undoubtedly be one of the primary sources of innovative CAR immune cell therapy design (Figure 2A).
Besides the receptor, engineering the cell host can improve its performance against cancer cells. Irving and colleagues summarize the concept of “coengineering”,9 highlighting the benefit of introducing multiple features besides the tumor-targeting receptor into immune cells to enhance their safety, specificity, and efficacy (Figure 2B). For instance, therapeutic antibodies (e.g., checkpoint inhibitors) or cytokines can be inducibly overexpressed in CAR T cells to enhance their proliferation and survival within the tumor microenvironment. In addition to gene overexpression, directly modifying the genome is an important coengineering approach. CRISPR/Cas has become the most essential tool in genome engineering. Chen and colleagues10 summarize the latest developments and experimental considerations in using CRISPR/Cas for unbiased functional screens in immune cells. They also discussed critical advances in creating more potent therapeutic immune cell therapies using CRISPR (Figure 2B). The ever-expanding capability of CRISPR technology will profoundly impact the understanding and development of immunotherapy.
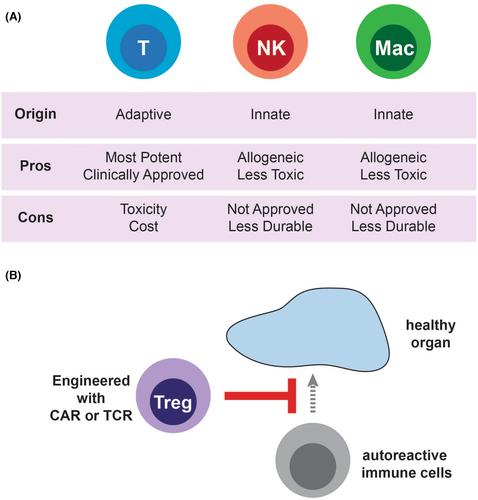
T cells are the primary cell type for creating CAR immune cell therapy. While T cells have proven to be a potent vehicle for CAR therapy, they also have shortcomings. One of the main challenges in using T cells is that they have a TCR, which leads to graft vs. host disease if the T cells are allogeneically sourced. As such, all clinically approved CAR T-cell therapies use T cells from the patient as the cell source. This drastically increases the complexity and cost of the manufacturing process. It is widely recognized that the next generation of immune cell therapy should be allogeneic or in situ engineered to ensure comprehensive patient access and commercial viability.
Deleting the TCR from the T-cell genome is one of the most prominent approaches to creating allogeneic CAR T cells. While intriguing, this approach also increases the manufacturing complexity. Therefore, other immune cell types with cell-killing capability that do not express a TCR are also being explored as potential vehicles for CAR. Natural killer (NK) cells are an intriguing alternative to T cells as the cell host because they have proven to be an essential player against cancer. Interestingly, the foundational CAR design also works in NK cells. In the review by Rezvani and colleagues,11 they highlight advances and understanding in CAR T and NK cells. Recent clinical trials with CAR NK cells have demonstrated exciting clinical efficacy with fewer side effects than CAR T cells. However, NK cells inherently have a shorter lifespan than T cells. Further advances in improving NK cell activity could pave the way for an off-the-shelf, allogeneic CAR immune cell therapy with activity comparable to T cells but with fewer side effects (Figure 3A).
In addition to T and NK cells, macrophages are also under investigation as a medium for immune cell therapy. Macrophages can naturally migrate into and accumulate in solid tumors, and many macrophages are routinely observed for various tumors. A modified CAR expressed in macrophages can induce antigen-dependent phagocytosis (Figure 3A). These properties make macrophages an attractive cell host for CAR. Our understanding of macrophage biology in the context of CAR is less than T cells. Gill and colleagues12 have prepared a review summarizing the opportunities and challenges of developing CAR macrophages as cancer immunotherapy. Due to their natural abundance and tumor-homing capability over other immune cell types, unlocking the potential of macrophages could have a significant manufacturing advantage.
Most applications of immune cell therapy are designed for treating cancer. However, engineered immune cells can also be leveraged to tackle autoimmunity and transplant rejection. Autoimmunity and transplant rejection are typically caused by immune cells, such as B and T cells, attacking the patient's healthy tissues or allografts. Only a small subset of B and T cells are auto- or alloreactive. Systemic immunosuppression is the current standard of care, but it is also accompanied by many complications and reduced capacity for the patient to fight infections. Using a CAR approach, CAR T cells have been designed to specifically eradicate only the autoreactive or alloreactive immune cells while sparing other healthy immune cells, thus providing a highly precise approach to address these unwanted immune responses without systemic immunosuppression. However, identifying the autoreactive and alloreactive B and T cells in autoimmune or transplant cases remains challenging. An alternative approach is to leverage regulatory T (Treg) cells, a subset of CD4 T cells that can suppress the immune response when the TCR signaling pathway is activated (Figure 3B). Unsurprisingly, CAR-expressing Treg can lead to antigen-dependent immune suppression. Levings and colleagues13 provide a detailed review of designer Treg's past achievements and current status. They also highlight the clinical potential of engineered Treg and discuss the ongoing preclinical studies and clinical trials on using designer Treg for various immune-mediated diseases.
We are now in the golden age of immunoengineering. The exciting and innovative immunoengineering developments summarized in this special issue of Immunological Reviews illustrate the immense potential that precise control over the immune system could have on developing disease-modifying, maybe even curative, therapies against some of the most untreatable diseases. These developments are, in part, accelerated by the convergence of multiple fields with immunology. For instance, the RNA technology that powers the unprecedented development of COVID vaccines is now being explored to create CAR T cells in situ, thus completely circumventing the need for cumbersome ex vivo cell processing. The main approach being investigated is to encapsulate messenger RNA (mRNA) encoding the gene of interest (e.g., CAR) into lipid nanoparticles and deliver the mRNA to immune cells inside the patient. The mRNA/LNP-based approach was recently leveraged to create CAR T cells against cardiac fibrotic tissues in mice to treat heart disease (PMID: 34990237).
Most conventional therapies aim to regulate one pathway or one cell type. However, that is different from how the therapy works in the complex, multicellular environment of a patient. For example, we learned from CAR T-cell therapy that we need both CD4 and CD8 T cells to be effective against cancer. Various combination therapies utilizing checkpoint inhibitors engage different parts of the immune response to elicit an efficacious response. Therefore, we anticipate that a purposeful modulation of multiple aspects of the immune system would further unlock the potential of immunotherapy. In addition, the immune response is a dynamic and carefully orchestrated process. We have seen that treating patients with chemotherapy to eliminate specific immune cells before administering CAR T cells could enhance their persistence and anti-cancer efficacy. Thus, considering the temporal order of multi-pronged regulation of the immune system could be the new dimension that can further accelerate the progress of immunotherapy.
W.W.W. holds equity in Senti Biosciences and 4Immune Therapeutics. W.A.L. holds equity in Gilead Sciences and Intellia Therapeutics and is an adviser for Allogene Therapeutics.
期刊介绍:
Immunological Reviews is a specialized journal that focuses on various aspects of immunological research. It encompasses a wide range of topics, such as clinical immunology, experimental immunology, and investigations related to allergy and the immune system.
The journal follows a unique approach where each volume is dedicated solely to a specific area of immunological research. However, collectively, these volumes aim to offer an extensive and up-to-date overview of the latest advancements in basic immunology and their practical implications in clinical settings.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


