Alan Cook, Rebecca Swindall, Katherine Spencer, Carly Wadle, S Andrew Cage, Musharaf Mohiuddin, Yagnesh Desai, Scott Norwood
{"title":"单水平下降后的住院和再入院:基于人群的样本。","authors":"Alan Cook, Rebecca Swindall, Katherine Spencer, Carly Wadle, S Andrew Cage, Musharaf Mohiuddin, Yagnesh Desai, Scott Norwood","doi":"10.1186/s40621-023-00463-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Single-level falls (SLFs) in the older US population is a leading cause of hospital admission and rates are increasing. Unscheduled hospital readmission is regarded as a quality-of-care indication and a preventable burden on healthcare systems. We aimed to characterize the predictors of 30-day readmission following admission for SLF injuries among patients 65 years and older.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study using the Nationwide Readmission Database from 2018 to 2019. Included patients were 65 and older, admitted emergently following a SLF with a primary injury diagnosis. Hierarchical logit regression was used to model factors associated with readmission within 30 days of discharge.</p><p><strong>Results: </strong>Of 1,338,905 trauma patients, 65 years or older, 61.3% had a single-level fall as the mechanism of injury. Among fallers, the average age was 81.1 years and 68.5% were female. SLF patients underwent more major therapeutic procedures (56.3% vs. 48.2%), spent over 2 million days in the hospital and incurred total charges of over $28 billion annually. Over 11% of SLF patients were readmitted within 30 days of discharge. Increasing income had a modest effect, where the highest zip code quartile was 9% less likely to be readmitted. Decreasing population density had a protective effect of readmission of 16%, comparing Non-Urban to Large Metropolitan. Transfer to short-term hospital, brain and vascular injuries were independent predictors of 30-day readmission in multivariable analysis (OR 2.50, 1.31, and 1.42, respectively). Palliative care consultation was protective (OR 0.41). The subsequent hospitalizations among those 30-day readmissions were primarily emergent (92.9%), consumed 260,876 hospital days and a total of $2.75 billion annually.</p><p><strong>Conclusions: </strong>SLFs exact costs to patients, health systems, and society. Transfer to short-term hospitals at discharge, along with brain and vascular injuries were strong predictors of 30-day readmission and warrant mitigation strategy development with consideration of expanded palliative care consultation.</p>","PeriodicalId":37379,"journal":{"name":"Injury Epidemiology","volume":"10 1","pages":"49"},"PeriodicalIF":2.4000,"publicationDate":"2023-10-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10588028/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hospitalization and readmission after single-level fall: a population-based sample.\",\"authors\":\"Alan Cook, Rebecca Swindall, Katherine Spencer, Carly Wadle, S Andrew Cage, Musharaf Mohiuddin, Yagnesh Desai, Scott Norwood\",\"doi\":\"10.1186/s40621-023-00463-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Single-level falls (SLFs) in the older US population is a leading cause of hospital admission and rates are increasing. Unscheduled hospital readmission is regarded as a quality-of-care indication and a preventable burden on healthcare systems. We aimed to characterize the predictors of 30-day readmission following admission for SLF injuries among patients 65 years and older.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study using the Nationwide Readmission Database from 2018 to 2019. Included patients were 65 and older, admitted emergently following a SLF with a primary injury diagnosis. Hierarchical logit regression was used to model factors associated with readmission within 30 days of discharge.</p><p><strong>Results: </strong>Of 1,338,905 trauma patients, 65 years or older, 61.3% had a single-level fall as the mechanism of injury. Among fallers, the average age was 81.1 years and 68.5% were female. SLF patients underwent more major therapeutic procedures (56.3% vs. 48.2%), spent over 2 million days in the hospital and incurred total charges of over $28 billion annually. Over 11% of SLF patients were readmitted within 30 days of discharge. Increasing income had a modest effect, where the highest zip code quartile was 9% less likely to be readmitted. Decreasing population density had a protective effect of readmission of 16%, comparing Non-Urban to Large Metropolitan. Transfer to short-term hospital, brain and vascular injuries were independent predictors of 30-day readmission in multivariable analysis (OR 2.50, 1.31, and 1.42, respectively). Palliative care consultation was protective (OR 0.41). The subsequent hospitalizations among those 30-day readmissions were primarily emergent (92.9%), consumed 260,876 hospital days and a total of $2.75 billion annually.</p><p><strong>Conclusions: </strong>SLFs exact costs to patients, health systems, and society. Transfer to short-term hospitals at discharge, along with brain and vascular injuries were strong predictors of 30-day readmission and warrant mitigation strategy development with consideration of expanded palliative care consultation.</p>\",\"PeriodicalId\":37379,\"journal\":{\"name\":\"Injury Epidemiology\",\"volume\":\"10 1\",\"pages\":\"49\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2023-10-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10588028/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Injury Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40621-023-00463-4\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Injury Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40621-023-00463-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Hospitalization and readmission after single-level fall: a population-based sample.
Background: Single-level falls (SLFs) in the older US population is a leading cause of hospital admission and rates are increasing. Unscheduled hospital readmission is regarded as a quality-of-care indication and a preventable burden on healthcare systems. We aimed to characterize the predictors of 30-day readmission following admission for SLF injuries among patients 65 years and older.
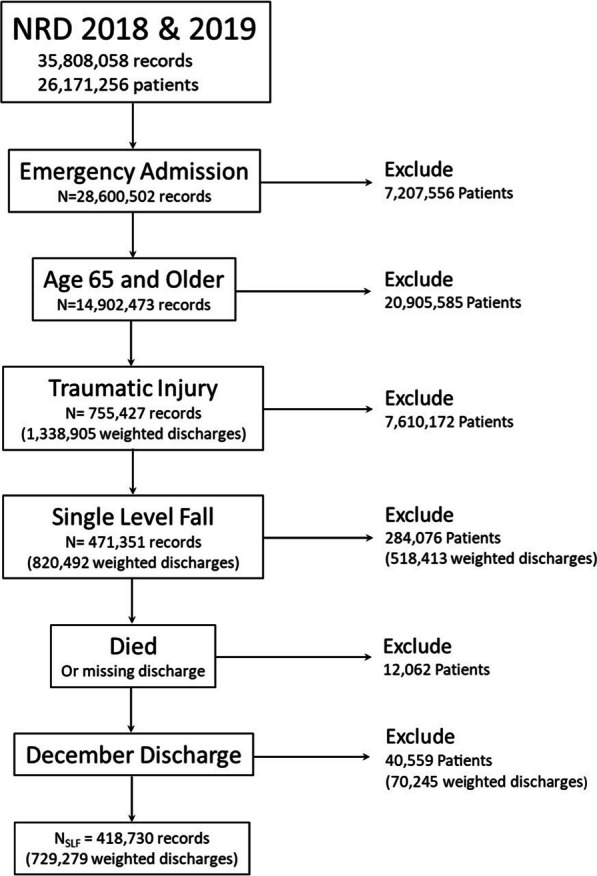
Methods: We conducted a retrospective cohort study using the Nationwide Readmission Database from 2018 to 2019. Included patients were 65 and older, admitted emergently following a SLF with a primary injury diagnosis. Hierarchical logit regression was used to model factors associated with readmission within 30 days of discharge.
Results: Of 1,338,905 trauma patients, 65 years or older, 61.3% had a single-level fall as the mechanism of injury. Among fallers, the average age was 81.1 years and 68.5% were female. SLF patients underwent more major therapeutic procedures (56.3% vs. 48.2%), spent over 2 million days in the hospital and incurred total charges of over $28 billion annually. Over 11% of SLF patients were readmitted within 30 days of discharge. Increasing income had a modest effect, where the highest zip code quartile was 9% less likely to be readmitted. Decreasing population density had a protective effect of readmission of 16%, comparing Non-Urban to Large Metropolitan. Transfer to short-term hospital, brain and vascular injuries were independent predictors of 30-day readmission in multivariable analysis (OR 2.50, 1.31, and 1.42, respectively). Palliative care consultation was protective (OR 0.41). The subsequent hospitalizations among those 30-day readmissions were primarily emergent (92.9%), consumed 260,876 hospital days and a total of $2.75 billion annually.
Conclusions: SLFs exact costs to patients, health systems, and society. Transfer to short-term hospitals at discharge, along with brain and vascular injuries were strong predictors of 30-day readmission and warrant mitigation strategy development with consideration of expanded palliative care consultation.
期刊介绍:
Injury Epidemiology is dedicated to advancing the scientific foundation for injury prevention and control through timely publication and dissemination of peer-reviewed research. Injury Epidemiology aims to be the premier venue for communicating epidemiologic studies of unintentional and intentional injuries, including, but not limited to, morbidity and mortality from motor vehicle crashes, drug overdose/poisoning, falls, drowning, fires/burns, iatrogenic injury, suicide, homicide, assaults, and abuse. We welcome investigations designed to understand the magnitude, distribution, determinants, causes, prevention, diagnosis, treatment, prognosis, and outcomes of injuries in specific population groups, geographic regions, and environmental settings (e.g., home, workplace, transport, recreation, sports, and urban/rural). Injury Epidemiology has a special focus on studies generating objective and practical knowledge that can be translated into interventions to reduce injury morbidity and mortality on a population level. Priority consideration will be given to manuscripts that feature contemporary theories and concepts, innovative methods, and novel techniques as applied to injury surveillance, risk assessment, development and implementation of effective interventions, and program and policy evaluation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


