{"title":"子宫切除术与甲状腺癌症风险的系统回顾和荟萃分析","authors":"Roberto Fabiani , Patrizia Rosignoli , Irene Giacchetta , Manuela Chiavarini","doi":"10.1016/j.gloepi.2023.100122","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Incidence rates of thyroid cancer have increased. Recent studies findings suggest that women who underwent a hysterectomy have an elevated relative risk of thyroid cancer. The aim of our meta-analysis is to summarize the evidence about the association between hysterectomy and thyroid cancer risk.</p></div><div><h3>Methods</h3><p>PubMed, Web of Science, and Scopus database were searched for studies published up to 5 September 2023. The PRISMA statement was followed. Heterogeneity was explored with Q statistic and the I2 statistic. Publication bias was assessed with Begg's and Egger's tests.</p></div><div><h3>Results</h3><p>Sixteen studies met the criteria. The pooled analysis showed a significantly 64% increment of thyroid cancer risk in association with any hysterectomy (OR 1.64, 95% CI 1.48–1.81; I2 = 28.68%, <em>p</em> = 0.156). Hysterectomy without oophorectomy was a stronger predictor of risk than hysterectomy with oophorectomy. The pooled analysis of data regarding hysterectomy without oophorectomy showed a statistically significant increment of thyroid cancer risk by 59%. Hysterectomy with oophorectomy was associated with an increase of thyroid cancer risk of 39% (OR 1.39, 95% CI 1.16–1.67; I2 = 42.10%, <em>p</em> = 0.049). Significant publication bias was not detected.</p></div><div><h3>Conclusions</h3><p>Our findings help with decision making around these surgeries.</p></div>","PeriodicalId":36311,"journal":{"name":"Global Epidemiology","volume":"6 ","pages":"Article 100122"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10582318/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hysterectomy and thyroid cancer risk: A systematic review and meta-analysis\",\"authors\":\"Roberto Fabiani , Patrizia Rosignoli , Irene Giacchetta , Manuela Chiavarini\",\"doi\":\"10.1016/j.gloepi.2023.100122\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Incidence rates of thyroid cancer have increased. Recent studies findings suggest that women who underwent a hysterectomy have an elevated relative risk of thyroid cancer. The aim of our meta-analysis is to summarize the evidence about the association between hysterectomy and thyroid cancer risk.</p></div><div><h3>Methods</h3><p>PubMed, Web of Science, and Scopus database were searched for studies published up to 5 September 2023. The PRISMA statement was followed. Heterogeneity was explored with Q statistic and the I2 statistic. Publication bias was assessed with Begg's and Egger's tests.</p></div><div><h3>Results</h3><p>Sixteen studies met the criteria. The pooled analysis showed a significantly 64% increment of thyroid cancer risk in association with any hysterectomy (OR 1.64, 95% CI 1.48–1.81; I2 = 28.68%, <em>p</em> = 0.156). Hysterectomy without oophorectomy was a stronger predictor of risk than hysterectomy with oophorectomy. The pooled analysis of data regarding hysterectomy without oophorectomy showed a statistically significant increment of thyroid cancer risk by 59%. Hysterectomy with oophorectomy was associated with an increase of thyroid cancer risk of 39% (OR 1.39, 95% CI 1.16–1.67; I2 = 42.10%, <em>p</em> = 0.049). Significant publication bias was not detected.</p></div><div><h3>Conclusions</h3><p>Our findings help with decision making around these surgeries.</p></div>\",\"PeriodicalId\":36311,\"journal\":{\"name\":\"Global Epidemiology\",\"volume\":\"6 \",\"pages\":\"Article 100122\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-10-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10582318/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Global Epidemiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590113323000251\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Epidemiology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590113323000251","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景癌症的发病率有所上升。最近的研究结果表明,接受子宫切除术的女性患甲状腺癌症的相对风险升高。我们的荟萃分析的目的是总结子宫切除术与甲状腺癌症风险之间的相关性证据。方法检索PubMed、Web of Science和Scopus数据库中截至2023年9月5日发表的研究。遵循了PRISMA的声明。利用Q统计量和I2统计量对异质性进行了探讨。发表偏倚通过Begg和Egger测试进行评估。结果16项研究符合标准。汇总分析显示,与任何子宫切除术相关的甲状腺癌症风险显著增加64%(OR 1.64,95%CI 1.48-1.81;I2=28.68%,p=0.156)。不经卵巢切除术的子宫切除术比经卵巢切除术的子宫切除手术更能预测风险。未经卵巢切除术的子宫切除术数据汇总分析显示,甲状腺癌症风险增加了59%,具有统计学意义。子宫切除术和卵巢切除术与甲状腺癌症风险增加39%相关(OR 1.39,95%CI 1.16–1.67;I2=42.10%,p=0.049)。未发现显著的发表偏倚。结论我们的研究结果有助于围绕这些手术做出决策。
Hysterectomy and thyroid cancer risk: A systematic review and meta-analysis
Background
Incidence rates of thyroid cancer have increased. Recent studies findings suggest that women who underwent a hysterectomy have an elevated relative risk of thyroid cancer. The aim of our meta-analysis is to summarize the evidence about the association between hysterectomy and thyroid cancer risk.
Methods
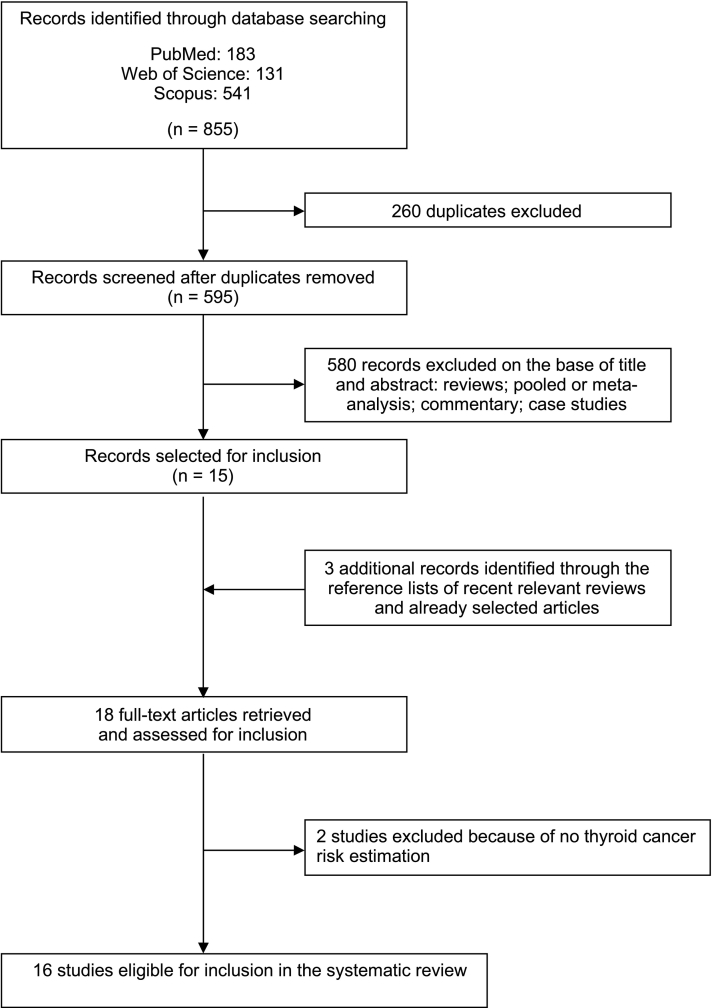
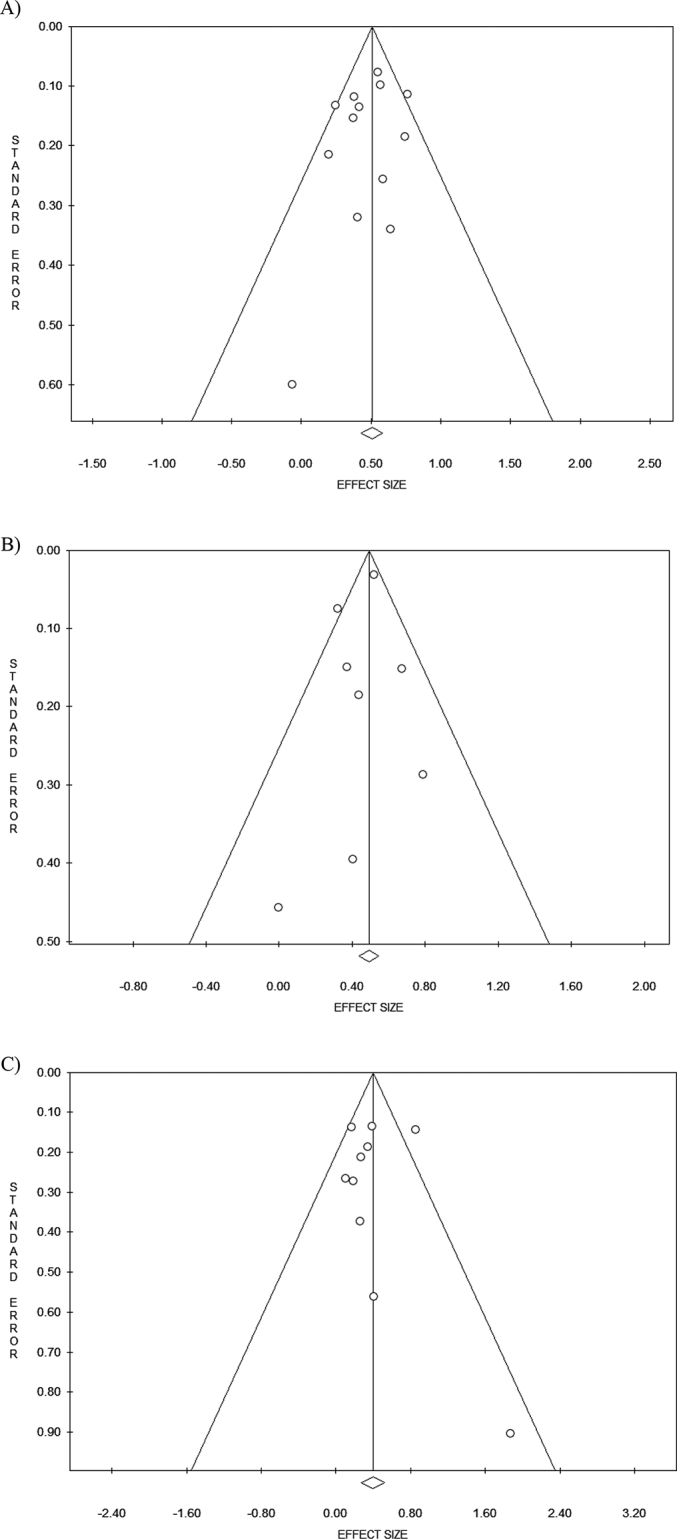
PubMed, Web of Science, and Scopus database were searched for studies published up to 5 September 2023. The PRISMA statement was followed. Heterogeneity was explored with Q statistic and the I2 statistic. Publication bias was assessed with Begg's and Egger's tests.
Results
Sixteen studies met the criteria. The pooled analysis showed a significantly 64% increment of thyroid cancer risk in association with any hysterectomy (OR 1.64, 95% CI 1.48–1.81; I2 = 28.68%, p = 0.156). Hysterectomy without oophorectomy was a stronger predictor of risk than hysterectomy with oophorectomy. The pooled analysis of data regarding hysterectomy without oophorectomy showed a statistically significant increment of thyroid cancer risk by 59%. Hysterectomy with oophorectomy was associated with an increase of thyroid cancer risk of 39% (OR 1.39, 95% CI 1.16–1.67; I2 = 42.10%, p = 0.049). Significant publication bias was not detected.
Conclusions
Our findings help with decision making around these surgeries.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


