Mark Peter Lythgoe, Maximilian Julve, David J. Pinato, Rohini Sharma
{"title":"瑞非尼治疗1例hiv -1感染患者的肝细胞癌1例报告","authors":"Mark Peter Lythgoe, Maximilian Julve, David J. Pinato, Rohini Sharma","doi":"10.1002/lci2.15","DOIUrl":null,"url":null,"abstract":"<p>The availability of safe, highly active anti-retroviral therapy (HAART) has dramatically ameliorated the morbidity related to human immunodeficiency virus (HIV) infection, significantly improving life expectancy.<span><sup>1</sup></span> A parallel reduction in AIDs-defining (acquired immunodeficiency syndrome) malignancies, such as Kaposi's sarcoma, primary central nervous system lymphoma and cervical cancer has also been observed.<span><sup>2</sup></span> Despite this reduction, rates of non-AIDs defining cancers including Hodgkin's lymphoma, anal cancer and hepatocellular carcinoma (HCC) have increased driven, at least in part, by improved overall survival.<span><sup>2</sup></span></p><p>The treatment armamentarium for advanced HCC has welcomed several new additions, with the development of multi-target tyrosine kinase inhibitors (TKIs) such as sorafenib and more recently lenvatinib, cabozantinib, regorafenib and the monoclonal antibody, ramucirumab.<span><sup>3-7</sup></span> The pivotal phase III RESORCE trial demonstrated regorafenib efficacy as a second-line treatment for BCLC stage B or C patients previously treated with sorafenib with preserved liver function (Child-Pugh A), improving overall survival by 3 months compared to placebo.<span><sup>6, 7</sup></span></p><p>Regulatory trials for these drugs, such as the RESORCE trial have excluded challenging patient populations, including those with concomitant HIV infection. This has led to uncertainly in terms of both safety and efficacy in these patient groups. Sorafenib has been licensed in the European Union since 2007. Following approval, evidence in the form of case reports/case series have demonstrated both the safety and utility of sorafenib in HIV-1 seropositive patients with advanced HCC.<span><sup>8, 9</sup></span> The concomitant use of HAART and sorafenib also appears to be both safe and effective.<span><sup>10</sup></span> However, for newer TKIs, such as regorafenib, there is currently no published evidence to guide safe administration.</p><p>This case report describes the first reported use of regorafenib in a patient with HIV-1 infection and advanced HCC.</p><p>A 68-year-old Nepalese gentleman with a history of HIV-1 infection and cirrhosis was diagnosed in July 2018 with multifocal HCC (largest lesion 6 cm) not amenable to curative treatment. The cirrhosis was attributed to heavy alcohol intake (~80 units/wk for >5 years) and was diagnosed following an episode of acute hepatic decompensation 4 years prior, involving variceal bleeding and encephalopathy. This resolved after conservative management and had not re-occurred following complete alcohol abstinence.</p><p>HIV-1 was diagnosed in 2011 following an episode of atypical pneumonia (presumed <i>Pneumocystis</i>). Tests for other viral infections, such as hepatitis B and C were negative. He was commenced on HAART at the time of diagnosis with Truvada<b><sup>®</sup></b> (Emtricitabine/Tenofovir) and Efavirenz. He had continued on this regimen uneventfully until his HCC diagnosis. His HIV-1 infection remained Centre for Disease Control (CDC) stage A (asymptomatic) with confirmatory blood tests showing a normal CD4 count (347 cells/μL) and undetectable viral load (<20 copies RNA/mL) at time of HCC diagnosis. His synthetic liver function was preserved (Child-Pugh A5) with albumin, bilirubin and prothrombin time within institutional normal limits. His alpha fetoprotein was 18 ng/mL.</p><p>Following multi-disciplinary review, he was deemed to be Barcelona Clinic Liver Cancer (BCLC) stage B. Loco-regional therapy was not feasible due to the multi-focal nature of the disease. A liver biopsy was deemed unnecessary as the imaging met diagnostic criteria for HCC. He was commenced on sorafenib 800 mg/daily. Following 6 weeks of treatment, he developed grade 2 diarrhoea and palmoplantar erythrodyaesthesia necessitating treatment suspension for 2 weeks and subsequent dose reduction to 400 mg/daily. Re-staging with triple-phase CT at 3-months confirmed stable disease (RECIST v1.1) and laboratory tests showed continued preservation of hepatic function (Child Pugh A5). He was maintained on treatment at the same dosage for a further 6 weeks, however upon clinical review described liver capsular pain and had increasing hepatomegaly. Subsequent imaging showed diffuse intrahepatic progressive disease at 5 months after sorafenib commencement, with the dominant lesion increasing in size to 7.5 cm (Figure 1A). Routine blood tests remained relatively unchanged with preserved synthetic liver function (Child Pugh A5) and stable alpha fetoprotein levels (19 ng/mL).</p><p>His HIV status precluded any clinical trial options. Given his excellent performance status (ECOG-0), preserved synthetic function (Child-Pugh A5) and strong motivation for treatment, consideration was given to using regorafenib as a second-line treatment.</p><p>Patients with HIV infection were excluded from the RESORCE trial, most likely due to concerns of disease and drug interactions. No specific drug-drug interactions have been recorded between regorafenib and HAART medications. However, both share common metabolic pathways via the cytochrome P450 enzyme system, specifically 3A4, which is of particular significance for non-nucleoside reverse transcription inhibitors, such as efavirenz. Current licensing recommendations include avoiding other potential CYP450 3A4 substrates (eg regorafenib) due to risk of precipitating serious adverse effects such as cardiac arrhythmias.<span><sup>11</sup></span> The development of HIV-1 integrase inhibitors, such as raltegravir represents an important therapeutic advance. These drugs offer an alternative hepatic metabolism independent of the CYP450 pathway, through UGT1A1 glucuronidation.<span><sup>12</sup></span> In this case, the patient was switched from efavirenz to raltegravir to avoid any potential drug-drug interactions.</p><p>After careful discussion with the patient regarding potential risks and benefits, an agreement was reached to commence on 160mg of regorafenib. The combination of HAART and regorafenib was well tolerated and after 3 months imaging showed stable disease with no deterioration in liver function (Child-Pugh A5). His HIV treatment remained unchanged, following a normal CD4 count (410 cells/μL) and undetectable viral load (<20 copies RNA/mL). Therefore, regorafenib was continued at the same dose.</p><p>Following 4 weeks of further treatment, he presented to clinic with new-onset confusion and grade 2 encephalopathy. Investigation revealed significant signs of hepatic decompensation with elevated bilirubin (51 μmol/L), prothrombin time (19.2 seconds) and reduced albumin (26 g/L). A plasma ammonia level (87 μmol/L) was also elevated. Due to his acute decompensation and that HIV seropositivity is associated with more aggressive HCC phenotype, urgent imaging was performed.<span><sup>13</sup></span> This confirmed disease progression with a significant increase in both the number and size of his HCC lesions (dominant lesion size increased to 8.5 cm, Figure 1B).</p><p>Confirmation of progressive disease necessitated treatment cessation. He was managed conservatively for his episode of decompensation, fully recovering over 4 weeks. Following this, he was transitioned to best supportive care as further treatment options (eg cabozantinib) are not reimbursed in the UK.<span><sup>14</sup></span> At the time of censoring (January 2020) he has been lost to follow-up. At his last clinical encounter (October 2019) he was engaged with community palliative care services and his HIV remains quiescent with an undetectable viral load (<20 copies RNA/mL).</p><p>Hepatocellular carcinoma has become an increasingly significant cause of HIV-related morbidity and mortality over the past decade.<span><sup>15</sup></span> HAART has led to the improved overall survival of HIV-infected individuals allowing time for HCC to develop, particularly in patients with risk factors such as viral hepatitis and excessive alcohol consumption.<span><sup>1</sup></span> Furthermore, preclinical models have demonstrated HIV may play a significant role in both viral and alcohol-induced hepatocarcinogenesis.<span><sup>16</sup></span></p><p>The licensing of sorafenib marked a paradigm shift in the treatment of advanced unresectable HCC. Utilizing regorafenib as a sequential treatment following sorafenib progression increases median overall survival by 7 months, compared to sorafenib treatment alone.<span><sup>6</sup></span> It is unknown how HIV seropositivity affects the pathogenesis of HCC. Studies have shown HIV-infected patients treated with sorafenib may have a shorter progression-free survival (PFS) and overall survival than seronegative patients.<span><sup>9, 13</sup></span> But the validity of this assertion is limited by the small patient numbers and retrospective nature of these studies. However, this case does support these previous findings, demonstrating a shortened PFS of only 4 months on sorafenib therapy. With regorafenib therapy the PFS was equivocal to that demonstrated in HIV seronegative patients.<span><sup>7</sup></span></p><p>The continued exclusion of patients with high predilection for developing HCC, such as HIV-infected individuals deprives this group of the potential benefit of therapeutic advances. This case study demonstrates that concomitant use of regorafenib and HAART was well tolerated and effective in a patient with concurrent HIV-1 and HCC.</p><p>Furthermore, as regorafenib is used in the management of other cancers, such as gastrointestinal stromal tumours (GISTs) and colorectal cancer, we hope this case provides additional insight into the potential safety of utilizing regorafenib with HAART universally. However, further ‘real world’ evidence and clinical studies are required to fully characterize clinical utility in this setting.</p>","PeriodicalId":93331,"journal":{"name":"Liver cancer international","volume":"1 2","pages":"51-54"},"PeriodicalIF":0.0000,"publicationDate":"2020-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/lci2.15","citationCount":"2","resultStr":"{\"title\":\"Regorafenib therapy for hepatocellular carcinoma in a HIV-1-infected patient: A case report\",\"authors\":\"Mark Peter Lythgoe, Maximilian Julve, David J. Pinato, Rohini Sharma\",\"doi\":\"10.1002/lci2.15\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The availability of safe, highly active anti-retroviral therapy (HAART) has dramatically ameliorated the morbidity related to human immunodeficiency virus (HIV) infection, significantly improving life expectancy.<span><sup>1</sup></span> A parallel reduction in AIDs-defining (acquired immunodeficiency syndrome) malignancies, such as Kaposi's sarcoma, primary central nervous system lymphoma and cervical cancer has also been observed.<span><sup>2</sup></span> Despite this reduction, rates of non-AIDs defining cancers including Hodgkin's lymphoma, anal cancer and hepatocellular carcinoma (HCC) have increased driven, at least in part, by improved overall survival.<span><sup>2</sup></span></p><p>The treatment armamentarium for advanced HCC has welcomed several new additions, with the development of multi-target tyrosine kinase inhibitors (TKIs) such as sorafenib and more recently lenvatinib, cabozantinib, regorafenib and the monoclonal antibody, ramucirumab.<span><sup>3-7</sup></span> The pivotal phase III RESORCE trial demonstrated regorafenib efficacy as a second-line treatment for BCLC stage B or C patients previously treated with sorafenib with preserved liver function (Child-Pugh A), improving overall survival by 3 months compared to placebo.<span><sup>6, 7</sup></span></p><p>Regulatory trials for these drugs, such as the RESORCE trial have excluded challenging patient populations, including those with concomitant HIV infection. This has led to uncertainly in terms of both safety and efficacy in these patient groups. Sorafenib has been licensed in the European Union since 2007. Following approval, evidence in the form of case reports/case series have demonstrated both the safety and utility of sorafenib in HIV-1 seropositive patients with advanced HCC.<span><sup>8, 9</sup></span> The concomitant use of HAART and sorafenib also appears to be both safe and effective.<span><sup>10</sup></span> However, for newer TKIs, such as regorafenib, there is currently no published evidence to guide safe administration.</p><p>This case report describes the first reported use of regorafenib in a patient with HIV-1 infection and advanced HCC.</p><p>A 68-year-old Nepalese gentleman with a history of HIV-1 infection and cirrhosis was diagnosed in July 2018 with multifocal HCC (largest lesion 6 cm) not amenable to curative treatment. The cirrhosis was attributed to heavy alcohol intake (~80 units/wk for >5 years) and was diagnosed following an episode of acute hepatic decompensation 4 years prior, involving variceal bleeding and encephalopathy. This resolved after conservative management and had not re-occurred following complete alcohol abstinence.</p><p>HIV-1 was diagnosed in 2011 following an episode of atypical pneumonia (presumed <i>Pneumocystis</i>). Tests for other viral infections, such as hepatitis B and C were negative. He was commenced on HAART at the time of diagnosis with Truvada<b><sup>®</sup></b> (Emtricitabine/Tenofovir) and Efavirenz. He had continued on this regimen uneventfully until his HCC diagnosis. His HIV-1 infection remained Centre for Disease Control (CDC) stage A (asymptomatic) with confirmatory blood tests showing a normal CD4 count (347 cells/μL) and undetectable viral load (<20 copies RNA/mL) at time of HCC diagnosis. His synthetic liver function was preserved (Child-Pugh A5) with albumin, bilirubin and prothrombin time within institutional normal limits. His alpha fetoprotein was 18 ng/mL.</p><p>Following multi-disciplinary review, he was deemed to be Barcelona Clinic Liver Cancer (BCLC) stage B. Loco-regional therapy was not feasible due to the multi-focal nature of the disease. A liver biopsy was deemed unnecessary as the imaging met diagnostic criteria for HCC. He was commenced on sorafenib 800 mg/daily. Following 6 weeks of treatment, he developed grade 2 diarrhoea and palmoplantar erythrodyaesthesia necessitating treatment suspension for 2 weeks and subsequent dose reduction to 400 mg/daily. Re-staging with triple-phase CT at 3-months confirmed stable disease (RECIST v1.1) and laboratory tests showed continued preservation of hepatic function (Child Pugh A5). He was maintained on treatment at the same dosage for a further 6 weeks, however upon clinical review described liver capsular pain and had increasing hepatomegaly. Subsequent imaging showed diffuse intrahepatic progressive disease at 5 months after sorafenib commencement, with the dominant lesion increasing in size to 7.5 cm (Figure 1A). Routine blood tests remained relatively unchanged with preserved synthetic liver function (Child Pugh A5) and stable alpha fetoprotein levels (19 ng/mL).</p><p>His HIV status precluded any clinical trial options. Given his excellent performance status (ECOG-0), preserved synthetic function (Child-Pugh A5) and strong motivation for treatment, consideration was given to using regorafenib as a second-line treatment.</p><p>Patients with HIV infection were excluded from the RESORCE trial, most likely due to concerns of disease and drug interactions. No specific drug-drug interactions have been recorded between regorafenib and HAART medications. However, both share common metabolic pathways via the cytochrome P450 enzyme system, specifically 3A4, which is of particular significance for non-nucleoside reverse transcription inhibitors, such as efavirenz. Current licensing recommendations include avoiding other potential CYP450 3A4 substrates (eg regorafenib) due to risk of precipitating serious adverse effects such as cardiac arrhythmias.<span><sup>11</sup></span> The development of HIV-1 integrase inhibitors, such as raltegravir represents an important therapeutic advance. These drugs offer an alternative hepatic metabolism independent of the CYP450 pathway, through UGT1A1 glucuronidation.<span><sup>12</sup></span> In this case, the patient was switched from efavirenz to raltegravir to avoid any potential drug-drug interactions.</p><p>After careful discussion with the patient regarding potential risks and benefits, an agreement was reached to commence on 160mg of regorafenib. The combination of HAART and regorafenib was well tolerated and after 3 months imaging showed stable disease with no deterioration in liver function (Child-Pugh A5). His HIV treatment remained unchanged, following a normal CD4 count (410 cells/μL) and undetectable viral load (<20 copies RNA/mL). Therefore, regorafenib was continued at the same dose.</p><p>Following 4 weeks of further treatment, he presented to clinic with new-onset confusion and grade 2 encephalopathy. Investigation revealed significant signs of hepatic decompensation with elevated bilirubin (51 μmol/L), prothrombin time (19.2 seconds) and reduced albumin (26 g/L). A plasma ammonia level (87 μmol/L) was also elevated. Due to his acute decompensation and that HIV seropositivity is associated with more aggressive HCC phenotype, urgent imaging was performed.<span><sup>13</sup></span> This confirmed disease progression with a significant increase in both the number and size of his HCC lesions (dominant lesion size increased to 8.5 cm, Figure 1B).</p><p>Confirmation of progressive disease necessitated treatment cessation. He was managed conservatively for his episode of decompensation, fully recovering over 4 weeks. Following this, he was transitioned to best supportive care as further treatment options (eg cabozantinib) are not reimbursed in the UK.<span><sup>14</sup></span> At the time of censoring (January 2020) he has been lost to follow-up. At his last clinical encounter (October 2019) he was engaged with community palliative care services and his HIV remains quiescent with an undetectable viral load (<20 copies RNA/mL).</p><p>Hepatocellular carcinoma has become an increasingly significant cause of HIV-related morbidity and mortality over the past decade.<span><sup>15</sup></span> HAART has led to the improved overall survival of HIV-infected individuals allowing time for HCC to develop, particularly in patients with risk factors such as viral hepatitis and excessive alcohol consumption.<span><sup>1</sup></span> Furthermore, preclinical models have demonstrated HIV may play a significant role in both viral and alcohol-induced hepatocarcinogenesis.<span><sup>16</sup></span></p><p>The licensing of sorafenib marked a paradigm shift in the treatment of advanced unresectable HCC. Utilizing regorafenib as a sequential treatment following sorafenib progression increases median overall survival by 7 months, compared to sorafenib treatment alone.<span><sup>6</sup></span> It is unknown how HIV seropositivity affects the pathogenesis of HCC. Studies have shown HIV-infected patients treated with sorafenib may have a shorter progression-free survival (PFS) and overall survival than seronegative patients.<span><sup>9, 13</sup></span> But the validity of this assertion is limited by the small patient numbers and retrospective nature of these studies. However, this case does support these previous findings, demonstrating a shortened PFS of only 4 months on sorafenib therapy. With regorafenib therapy the PFS was equivocal to that demonstrated in HIV seronegative patients.<span><sup>7</sup></span></p><p>The continued exclusion of patients with high predilection for developing HCC, such as HIV-infected individuals deprives this group of the potential benefit of therapeutic advances. This case study demonstrates that concomitant use of regorafenib and HAART was well tolerated and effective in a patient with concurrent HIV-1 and HCC.</p><p>Furthermore, as regorafenib is used in the management of other cancers, such as gastrointestinal stromal tumours (GISTs) and colorectal cancer, we hope this case provides additional insight into the potential safety of utilizing regorafenib with HAART universally. However, further ‘real world’ evidence and clinical studies are required to fully characterize clinical utility in this setting.</p>\",\"PeriodicalId\":93331,\"journal\":{\"name\":\"Liver cancer international\",\"volume\":\"1 2\",\"pages\":\"51-54\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-06-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/lci2.15\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Liver cancer international\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/lci2.15\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Liver cancer international","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lci2.15","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Regorafenib therapy for hepatocellular carcinoma in a HIV-1-infected patient: A case report
The availability of safe, highly active anti-retroviral therapy (HAART) has dramatically ameliorated the morbidity related to human immunodeficiency virus (HIV) infection, significantly improving life expectancy.1 A parallel reduction in AIDs-defining (acquired immunodeficiency syndrome) malignancies, such as Kaposi's sarcoma, primary central nervous system lymphoma and cervical cancer has also been observed.2 Despite this reduction, rates of non-AIDs defining cancers including Hodgkin's lymphoma, anal cancer and hepatocellular carcinoma (HCC) have increased driven, at least in part, by improved overall survival.2
The treatment armamentarium for advanced HCC has welcomed several new additions, with the development of multi-target tyrosine kinase inhibitors (TKIs) such as sorafenib and more recently lenvatinib, cabozantinib, regorafenib and the monoclonal antibody, ramucirumab.3-7 The pivotal phase III RESORCE trial demonstrated regorafenib efficacy as a second-line treatment for BCLC stage B or C patients previously treated with sorafenib with preserved liver function (Child-Pugh A), improving overall survival by 3 months compared to placebo.6, 7
Regulatory trials for these drugs, such as the RESORCE trial have excluded challenging patient populations, including those with concomitant HIV infection. This has led to uncertainly in terms of both safety and efficacy in these patient groups. Sorafenib has been licensed in the European Union since 2007. Following approval, evidence in the form of case reports/case series have demonstrated both the safety and utility of sorafenib in HIV-1 seropositive patients with advanced HCC.8, 9 The concomitant use of HAART and sorafenib also appears to be both safe and effective.10 However, for newer TKIs, such as regorafenib, there is currently no published evidence to guide safe administration.
This case report describes the first reported use of regorafenib in a patient with HIV-1 infection and advanced HCC.
A 68-year-old Nepalese gentleman with a history of HIV-1 infection and cirrhosis was diagnosed in July 2018 with multifocal HCC (largest lesion 6 cm) not amenable to curative treatment. The cirrhosis was attributed to heavy alcohol intake (~80 units/wk for >5 years) and was diagnosed following an episode of acute hepatic decompensation 4 years prior, involving variceal bleeding and encephalopathy. This resolved after conservative management and had not re-occurred following complete alcohol abstinence.
HIV-1 was diagnosed in 2011 following an episode of atypical pneumonia (presumed Pneumocystis). Tests for other viral infections, such as hepatitis B and C were negative. He was commenced on HAART at the time of diagnosis with Truvada® (Emtricitabine/Tenofovir) and Efavirenz. He had continued on this regimen uneventfully until his HCC diagnosis. His HIV-1 infection remained Centre for Disease Control (CDC) stage A (asymptomatic) with confirmatory blood tests showing a normal CD4 count (347 cells/μL) and undetectable viral load (<20 copies RNA/mL) at time of HCC diagnosis. His synthetic liver function was preserved (Child-Pugh A5) with albumin, bilirubin and prothrombin time within institutional normal limits. His alpha fetoprotein was 18 ng/mL.
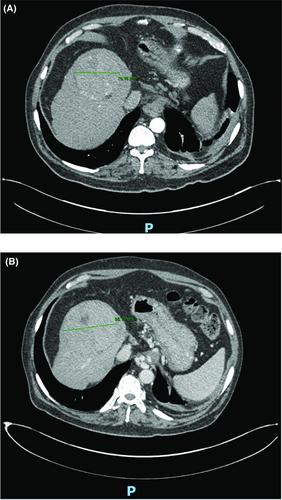
Following multi-disciplinary review, he was deemed to be Barcelona Clinic Liver Cancer (BCLC) stage B. Loco-regional therapy was not feasible due to the multi-focal nature of the disease. A liver biopsy was deemed unnecessary as the imaging met diagnostic criteria for HCC. He was commenced on sorafenib 800 mg/daily. Following 6 weeks of treatment, he developed grade 2 diarrhoea and palmoplantar erythrodyaesthesia necessitating treatment suspension for 2 weeks and subsequent dose reduction to 400 mg/daily. Re-staging with triple-phase CT at 3-months confirmed stable disease (RECIST v1.1) and laboratory tests showed continued preservation of hepatic function (Child Pugh A5). He was maintained on treatment at the same dosage for a further 6 weeks, however upon clinical review described liver capsular pain and had increasing hepatomegaly. Subsequent imaging showed diffuse intrahepatic progressive disease at 5 months after sorafenib commencement, with the dominant lesion increasing in size to 7.5 cm (Figure 1A). Routine blood tests remained relatively unchanged with preserved synthetic liver function (Child Pugh A5) and stable alpha fetoprotein levels (19 ng/mL).
His HIV status precluded any clinical trial options. Given his excellent performance status (ECOG-0), preserved synthetic function (Child-Pugh A5) and strong motivation for treatment, consideration was given to using regorafenib as a second-line treatment.
Patients with HIV infection were excluded from the RESORCE trial, most likely due to concerns of disease and drug interactions. No specific drug-drug interactions have been recorded between regorafenib and HAART medications. However, both share common metabolic pathways via the cytochrome P450 enzyme system, specifically 3A4, which is of particular significance for non-nucleoside reverse transcription inhibitors, such as efavirenz. Current licensing recommendations include avoiding other potential CYP450 3A4 substrates (eg regorafenib) due to risk of precipitating serious adverse effects such as cardiac arrhythmias.11 The development of HIV-1 integrase inhibitors, such as raltegravir represents an important therapeutic advance. These drugs offer an alternative hepatic metabolism independent of the CYP450 pathway, through UGT1A1 glucuronidation.12 In this case, the patient was switched from efavirenz to raltegravir to avoid any potential drug-drug interactions.
After careful discussion with the patient regarding potential risks and benefits, an agreement was reached to commence on 160mg of regorafenib. The combination of HAART and regorafenib was well tolerated and after 3 months imaging showed stable disease with no deterioration in liver function (Child-Pugh A5). His HIV treatment remained unchanged, following a normal CD4 count (410 cells/μL) and undetectable viral load (<20 copies RNA/mL). Therefore, regorafenib was continued at the same dose.
Following 4 weeks of further treatment, he presented to clinic with new-onset confusion and grade 2 encephalopathy. Investigation revealed significant signs of hepatic decompensation with elevated bilirubin (51 μmol/L), prothrombin time (19.2 seconds) and reduced albumin (26 g/L). A plasma ammonia level (87 μmol/L) was also elevated. Due to his acute decompensation and that HIV seropositivity is associated with more aggressive HCC phenotype, urgent imaging was performed.13 This confirmed disease progression with a significant increase in both the number and size of his HCC lesions (dominant lesion size increased to 8.5 cm, Figure 1B).
Confirmation of progressive disease necessitated treatment cessation. He was managed conservatively for his episode of decompensation, fully recovering over 4 weeks. Following this, he was transitioned to best supportive care as further treatment options (eg cabozantinib) are not reimbursed in the UK.14 At the time of censoring (January 2020) he has been lost to follow-up. At his last clinical encounter (October 2019) he was engaged with community palliative care services and his HIV remains quiescent with an undetectable viral load (<20 copies RNA/mL).
Hepatocellular carcinoma has become an increasingly significant cause of HIV-related morbidity and mortality over the past decade.15 HAART has led to the improved overall survival of HIV-infected individuals allowing time for HCC to develop, particularly in patients with risk factors such as viral hepatitis and excessive alcohol consumption.1 Furthermore, preclinical models have demonstrated HIV may play a significant role in both viral and alcohol-induced hepatocarcinogenesis.16
The licensing of sorafenib marked a paradigm shift in the treatment of advanced unresectable HCC. Utilizing regorafenib as a sequential treatment following sorafenib progression increases median overall survival by 7 months, compared to sorafenib treatment alone.6 It is unknown how HIV seropositivity affects the pathogenesis of HCC. Studies have shown HIV-infected patients treated with sorafenib may have a shorter progression-free survival (PFS) and overall survival than seronegative patients.9, 13 But the validity of this assertion is limited by the small patient numbers and retrospective nature of these studies. However, this case does support these previous findings, demonstrating a shortened PFS of only 4 months on sorafenib therapy. With regorafenib therapy the PFS was equivocal to that demonstrated in HIV seronegative patients.7
The continued exclusion of patients with high predilection for developing HCC, such as HIV-infected individuals deprives this group of the potential benefit of therapeutic advances. This case study demonstrates that concomitant use of regorafenib and HAART was well tolerated and effective in a patient with concurrent HIV-1 and HCC.
Furthermore, as regorafenib is used in the management of other cancers, such as gastrointestinal stromal tumours (GISTs) and colorectal cancer, we hope this case provides additional insight into the potential safety of utilizing regorafenib with HAART universally. However, further ‘real world’ evidence and clinical studies are required to fully characterize clinical utility in this setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


