{"title":"铋配合标准三联疗法与联合疗法的个性化治疗:幽门螺杆菌感染的一线方案","authors":"Soo Yeon Choi, Na Rae Lim, Woo Chul Chung","doi":"10.7704/kjhugr.2022.0058","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aims: </strong>Compared with other regimens, concomitant therapy (CT) used as a first-line regimen for <i>Helicobacter pylori (H. pylori)</i> infection is associated with higher eradication rates. We compared the efficacy of tailored therapy (TT) using bismuth added to standard triple therapy (STT) with CT.</p><p><strong>Methods: </strong>This consecutive study performed between September 2020 and 2021 included 210 patients with <i>H. pylori</i> infection. Two participating gastroenterologists prescribed TT and CT. Multiplex PCR assays were performed before eradication therapy to identify the relevant point mutations and confirm clarithromycin resistance in the TT group (n=105). Patients who showed negative PCR results received 14-day STT and those with positive PCR results received a 14-day regimen of bismuth added to STT. The other group (n=105) received 10-day CT.</p><p><strong>Results: </strong>Based on per-protocol analysis, eradication rates in the TT and CT groups were 89.2% (91/102) and 81.6% (84/103), respectively. We observed no statistically significant intergroup differences in eradication rates (<i>P</i>=0.12). The frequency of estimated clarithromycin resistance confirmed using multiplex PCR assays was 32.4% (34/105), and the eradication rate associated with bismuth add-on STT was 76.5% (26/34) in patients with clarithromycin resistance.</p><p><strong>Conclusions: </strong>Considering the current and emerging trends in antibiotic resistance, a therapeutic strategy using TT (bismuth add-on STT) is recommended to minimize unnecessary administration of antibiotics.</p>","PeriodicalId":22895,"journal":{"name":"The Korean Journal of Helicobacter and Upper Gastrointestinal Research","volume":" ","pages":"118-124"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11967524/pdf/","citationCount":"0","resultStr":"{\"title\":\"Tailored Therapy Using Bismuth Add-on Standard Triple Therapy vs. Concomitant Therapy: A First-line Regimen for <i>Helicobacter pylori</i> Infection.\",\"authors\":\"Soo Yeon Choi, Na Rae Lim, Woo Chul Chung\",\"doi\":\"10.7704/kjhugr.2022.0058\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/aims: </strong>Compared with other regimens, concomitant therapy (CT) used as a first-line regimen for <i>Helicobacter pylori (H. pylori)</i> infection is associated with higher eradication rates. We compared the efficacy of tailored therapy (TT) using bismuth added to standard triple therapy (STT) with CT.</p><p><strong>Methods: </strong>This consecutive study performed between September 2020 and 2021 included 210 patients with <i>H. pylori</i> infection. Two participating gastroenterologists prescribed TT and CT. Multiplex PCR assays were performed before eradication therapy to identify the relevant point mutations and confirm clarithromycin resistance in the TT group (n=105). Patients who showed negative PCR results received 14-day STT and those with positive PCR results received a 14-day regimen of bismuth added to STT. The other group (n=105) received 10-day CT.</p><p><strong>Results: </strong>Based on per-protocol analysis, eradication rates in the TT and CT groups were 89.2% (91/102) and 81.6% (84/103), respectively. We observed no statistically significant intergroup differences in eradication rates (<i>P</i>=0.12). The frequency of estimated clarithromycin resistance confirmed using multiplex PCR assays was 32.4% (34/105), and the eradication rate associated with bismuth add-on STT was 76.5% (26/34) in patients with clarithromycin resistance.</p><p><strong>Conclusions: </strong>Considering the current and emerging trends in antibiotic resistance, a therapeutic strategy using TT (bismuth add-on STT) is recommended to minimize unnecessary administration of antibiotics.</p>\",\"PeriodicalId\":22895,\"journal\":{\"name\":\"The Korean Journal of Helicobacter and Upper Gastrointestinal Research\",\"volume\":\" \",\"pages\":\"118-124\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11967524/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Korean Journal of Helicobacter and Upper Gastrointestinal Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7704/kjhugr.2022.0058\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/4/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Korean Journal of Helicobacter and Upper Gastrointestinal Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7704/kjhugr.2022.0058","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/10 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Tailored Therapy Using Bismuth Add-on Standard Triple Therapy vs. Concomitant Therapy: A First-line Regimen for Helicobacter pylori Infection.
Background/aims: Compared with other regimens, concomitant therapy (CT) used as a first-line regimen for Helicobacter pylori (H. pylori) infection is associated with higher eradication rates. We compared the efficacy of tailored therapy (TT) using bismuth added to standard triple therapy (STT) with CT.
Methods: This consecutive study performed between September 2020 and 2021 included 210 patients with H. pylori infection. Two participating gastroenterologists prescribed TT and CT. Multiplex PCR assays were performed before eradication therapy to identify the relevant point mutations and confirm clarithromycin resistance in the TT group (n=105). Patients who showed negative PCR results received 14-day STT and those with positive PCR results received a 14-day regimen of bismuth added to STT. The other group (n=105) received 10-day CT.
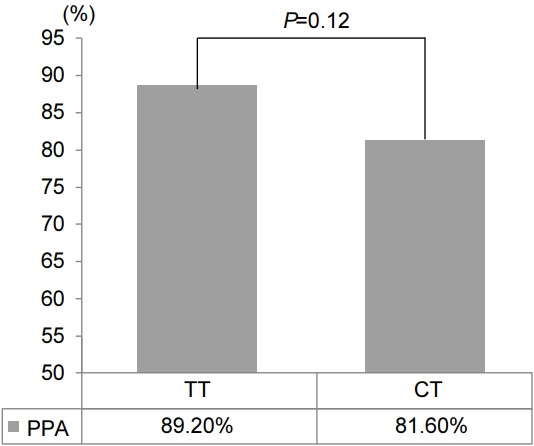
Results: Based on per-protocol analysis, eradication rates in the TT and CT groups were 89.2% (91/102) and 81.6% (84/103), respectively. We observed no statistically significant intergroup differences in eradication rates (P=0.12). The frequency of estimated clarithromycin resistance confirmed using multiplex PCR assays was 32.4% (34/105), and the eradication rate associated with bismuth add-on STT was 76.5% (26/34) in patients with clarithromycin resistance.
Conclusions: Considering the current and emerging trends in antibiotic resistance, a therapeutic strategy using TT (bismuth add-on STT) is recommended to minimize unnecessary administration of antibiotics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


