Kirstine N la Cour, Nina C Andersen-Ranberg, Sarah Weihe, Lone M Poulsen, Camilla B Mortensen, Cilia K W Kjer, Marie O Collet, Stine Estrup, Ole Mathiesen
{"title":"重症监护病房谵妄运动亚型的分布:一项系统的范围审查","authors":"Kirstine N la Cour, Nina C Andersen-Ranberg, Sarah Weihe, Lone M Poulsen, Camilla B Mortensen, Cilia K W Kjer, Marie O Collet, Stine Estrup, Ole Mathiesen","doi":"10.1186/s13054-022-03931-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Delirium is the most common cerebral dysfunction in the intensive care unit (ICU) and can be subdivided into a hypoactive, hyperactive, or mixed motor subtype based on the clinical manifestation. The aim of this review was to describe the distribution, pharmacological interventions, and outcomes of delirium motor subtypes in ICU patients.</p><p><strong>Methods: </strong>This systematic scoping review was performed according to the PRISMA-ScR and Cochrane guidelines. We performed a systematic search in six major databases to identify relevant studies. A meta-regression analysis was performed where pooled estimates with 95% confidence intervals were computed by a random effect model.</p><p><strong>Results: </strong>We included 131 studies comprising 13,902 delirious patients. There was a large between-study heterogeneity among studies, including differences in study design, setting, population, and outcome reporting. Hypoactive delirium was the most prevalent delirium motor subtype (50.3% [95% CI 46.0-54.7]), followed by mixed delirium (27.7% [95% CI 24.1-31.3]) and hyperactive delirium (22.7% [95% CI 19.0-26.5]). When comparing the delirium motor subtypes, patients with mixed delirium experienced the longest delirium duration, ICU and hospital length of stay, the highest ICU and hospital mortality, and more frequently received administration of specific agents (antipsychotics, α2-agonists, benzodiazepines, and propofol) during ICU stay. In studies with high average age for delirious patients (> 65 years), patients were more likely to experience hypoactive delirium.</p><p><strong>Conclusions: </strong>Hypoactive delirium was the most prevalent motor subtype in critically ill patients. Mixed delirium had the worst outcomes in terms of delirium duration, length of stay, and mortality, and received more pharmacological interventions compared to other delirium motor subtypes. Few studies contributed to secondary outcomes; hence, these results should be interpreted with care. The large between-study heterogeneity suggests that a more standardized methodology in delirium research is warranted.</p>","PeriodicalId":92888,"journal":{"name":"Critical care (Houten, Netherlands)","volume":" ","pages":"53"},"PeriodicalIF":0.0000,"publicationDate":"2022-03-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8896322/pdf/","citationCount":"0","resultStr":"{\"title\":\"Distribution of delirium motor subtypes in the intensive care unit: a systematic scoping review.\",\"authors\":\"Kirstine N la Cour, Nina C Andersen-Ranberg, Sarah Weihe, Lone M Poulsen, Camilla B Mortensen, Cilia K W Kjer, Marie O Collet, Stine Estrup, Ole Mathiesen\",\"doi\":\"10.1186/s13054-022-03931-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Delirium is the most common cerebral dysfunction in the intensive care unit (ICU) and can be subdivided into a hypoactive, hyperactive, or mixed motor subtype based on the clinical manifestation. The aim of this review was to describe the distribution, pharmacological interventions, and outcomes of delirium motor subtypes in ICU patients.</p><p><strong>Methods: </strong>This systematic scoping review was performed according to the PRISMA-ScR and Cochrane guidelines. We performed a systematic search in six major databases to identify relevant studies. A meta-regression analysis was performed where pooled estimates with 95% confidence intervals were computed by a random effect model.</p><p><strong>Results: </strong>We included 131 studies comprising 13,902 delirious patients. There was a large between-study heterogeneity among studies, including differences in study design, setting, population, and outcome reporting. Hypoactive delirium was the most prevalent delirium motor subtype (50.3% [95% CI 46.0-54.7]), followed by mixed delirium (27.7% [95% CI 24.1-31.3]) and hyperactive delirium (22.7% [95% CI 19.0-26.5]). When comparing the delirium motor subtypes, patients with mixed delirium experienced the longest delirium duration, ICU and hospital length of stay, the highest ICU and hospital mortality, and more frequently received administration of specific agents (antipsychotics, α2-agonists, benzodiazepines, and propofol) during ICU stay. In studies with high average age for delirious patients (> 65 years), patients were more likely to experience hypoactive delirium.</p><p><strong>Conclusions: </strong>Hypoactive delirium was the most prevalent motor subtype in critically ill patients. Mixed delirium had the worst outcomes in terms of delirium duration, length of stay, and mortality, and received more pharmacological interventions compared to other delirium motor subtypes. Few studies contributed to secondary outcomes; hence, these results should be interpreted with care. The large between-study heterogeneity suggests that a more standardized methodology in delirium research is warranted.</p>\",\"PeriodicalId\":92888,\"journal\":{\"name\":\"Critical care (Houten, Netherlands)\",\"volume\":\" \",\"pages\":\"53\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-03-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8896322/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care (Houten, Netherlands)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13054-022-03931-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care (Houten, Netherlands)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13054-022-03931-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:谵妄是重症监护病房(ICU)最常见的脑功能障碍,根据临床表现可分为低动型、多动型或混合运动型。本综述的目的是描述ICU患者谵妄运动亚型的分布、药物干预和结局。方法:根据PRISMA-ScR和Cochrane指南进行系统的范围评价。我们在六个主要数据库中进行了系统检索,以确定相关研究。通过随机效应模型计算95%置信区间的汇总估计,进行meta回归分析。结果:我们纳入131项研究,包括13902名谵妄患者。研究之间存在较大的研究间异质性,包括研究设计、环境、人群和结果报告的差异。谵妄运动亚型以低活动性谵妄最为常见(50.3% [95% CI 46.0 ~ 54.7]),其次为混合性谵妄(27.7% [95% CI 24.1 ~ 31.3])和多活动性谵妄(22.7% [95% CI 19.0 ~ 26.5])。在比较谵妄运动亚型时,混合性谵妄患者谵妄持续时间最长,ICU和住院时间最长,ICU和住院死亡率最高,并且在ICU住院期间使用特定药物(抗精神病药物、α2激动剂、苯二氮卓类药物和异丙酚)的频率更高。在研究中,谵妄患者的平均年龄较高(约65岁),患者更容易出现低活动性谵妄。结论:低活动性谵妄是危重症患者最常见的运动亚型。混合性谵妄在谵妄持续时间、住院时间和死亡率方面的预后最差,与其他谵妄运动亚型相比,混合性谵妄接受了更多的药物干预。很少有研究对次要结局有贡献;因此,这些结果应该谨慎解释。研究间的巨大异质性表明,在谵妄研究中有必要采用更标准化的方法。
Distribution of delirium motor subtypes in the intensive care unit: a systematic scoping review.
Background: Delirium is the most common cerebral dysfunction in the intensive care unit (ICU) and can be subdivided into a hypoactive, hyperactive, or mixed motor subtype based on the clinical manifestation. The aim of this review was to describe the distribution, pharmacological interventions, and outcomes of delirium motor subtypes in ICU patients.
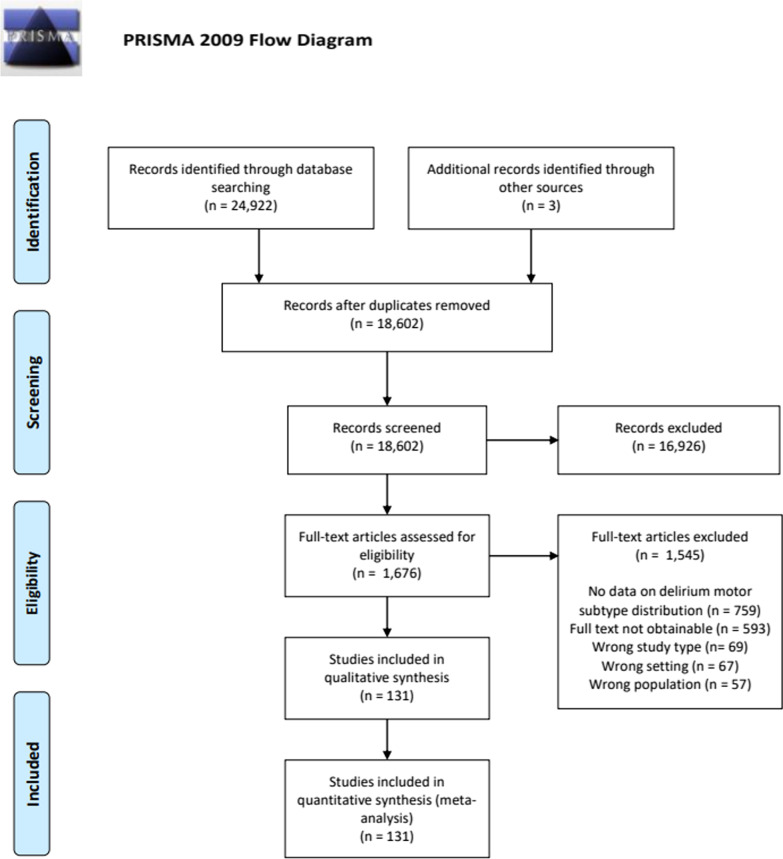
Methods: This systematic scoping review was performed according to the PRISMA-ScR and Cochrane guidelines. We performed a systematic search in six major databases to identify relevant studies. A meta-regression analysis was performed where pooled estimates with 95% confidence intervals were computed by a random effect model.
Results: We included 131 studies comprising 13,902 delirious patients. There was a large between-study heterogeneity among studies, including differences in study design, setting, population, and outcome reporting. Hypoactive delirium was the most prevalent delirium motor subtype (50.3% [95% CI 46.0-54.7]), followed by mixed delirium (27.7% [95% CI 24.1-31.3]) and hyperactive delirium (22.7% [95% CI 19.0-26.5]). When comparing the delirium motor subtypes, patients with mixed delirium experienced the longest delirium duration, ICU and hospital length of stay, the highest ICU and hospital mortality, and more frequently received administration of specific agents (antipsychotics, α2-agonists, benzodiazepines, and propofol) during ICU stay. In studies with high average age for delirious patients (> 65 years), patients were more likely to experience hypoactive delirium.
Conclusions: Hypoactive delirium was the most prevalent motor subtype in critically ill patients. Mixed delirium had the worst outcomes in terms of delirium duration, length of stay, and mortality, and received more pharmacological interventions compared to other delirium motor subtypes. Few studies contributed to secondary outcomes; hence, these results should be interpreted with care. The large between-study heterogeneity suggests that a more standardized methodology in delirium research is warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


