{"title":"基于列线图的院前急性缺血性脑卒中筛查临床工具","authors":"Alireza Baratloo, Mahtab Ramezani, Hosein Rafiemanesh, Meisam Sharifi, Somayeh Karimi","doi":"10.18502/cjn.v22i1.12618","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> We believe that designing a new tool which is comparable in terms of both sensitivity and specificity may play an important role in rapid and more accurate diagnosis of acute ischemic stroke (AIS) in prehospital stage. Therefore, we intended to develop a new clinical tool for the diagnosis of AIS in the prehospital stage. <b>Methods:</b> This was a cross-sectional diagnostic accuracy study. All patients transferred to the emergency department (ED) who underwent brain magnetic resonance imaging (MRI) with impression of AIS were evaluated by 9 clinical tools for stroke diagnosis in the pre-hospital phase including Rapid Arterial Occlusion Evaluation (RACE), Cincinnati Prehospital Stroke Scale (CPSS), Los Angeles Prehospital Stroke Screen (LAPSS), Melbourne Ambulance Stroke Screen (MASS), Medic Prehospital Assessment for Code Stroke (Med PACS), Ontario Prehospital Stroke Screening Tool (OPSS), PreHospital Ambulance Stroke Test (PreHAST), Recognition of Stroke in the Emergency Room (ROSIER), and Face Arm Speech Test (FAST), and totally 19 items were reviewed and recorded. The new clinical tool was developed based on backward method of multivariable logistic regression analysis. The discrimination power of the new clinical tool for diagnosis of AIS was assessed with the area under the receiver operating characteristic curve (AUC-ROC). <b>Results:</b> Data from 806 patients were analyzed; of them, 57.4% were men. The mean age of the study patients was 66.9 years [standard deviation (SD) = 13.9]. In the multivariable model, 8 items remained. The AUC-ROC of the new clinical tool was 0.893 [95% confidence interval (CI): 0.869-0.917], and its best cut-off point was score ≥ 3 for positive AIS. At this cut-off point, sensitivity and specificity were 84.42% and 79.72%, respectively. <b>Conclusion:</b> We introduced a new nomogram-based clinical tool for the diagnosis of AIS in the prehospital stage, which has acceptable specificity and sensitivity; moreover, it is comparable with previous tools.</p>","PeriodicalId":40077,"journal":{"name":"Current Journal of Neurology","volume":"22 1","pages":"58-62"},"PeriodicalIF":0.5000,"publicationDate":"2023-01-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10444598/pdf/","citationCount":"0","resultStr":"{\"title\":\"A nomogram-based clinical tool for acute ischemic stroke screening in prehospital setting.\",\"authors\":\"Alireza Baratloo, Mahtab Ramezani, Hosein Rafiemanesh, Meisam Sharifi, Somayeh Karimi\",\"doi\":\"10.18502/cjn.v22i1.12618\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> We believe that designing a new tool which is comparable in terms of both sensitivity and specificity may play an important role in rapid and more accurate diagnosis of acute ischemic stroke (AIS) in prehospital stage. Therefore, we intended to develop a new clinical tool for the diagnosis of AIS in the prehospital stage. <b>Methods:</b> This was a cross-sectional diagnostic accuracy study. All patients transferred to the emergency department (ED) who underwent brain magnetic resonance imaging (MRI) with impression of AIS were evaluated by 9 clinical tools for stroke diagnosis in the pre-hospital phase including Rapid Arterial Occlusion Evaluation (RACE), Cincinnati Prehospital Stroke Scale (CPSS), Los Angeles Prehospital Stroke Screen (LAPSS), Melbourne Ambulance Stroke Screen (MASS), Medic Prehospital Assessment for Code Stroke (Med PACS), Ontario Prehospital Stroke Screening Tool (OPSS), PreHospital Ambulance Stroke Test (PreHAST), Recognition of Stroke in the Emergency Room (ROSIER), and Face Arm Speech Test (FAST), and totally 19 items were reviewed and recorded. The new clinical tool was developed based on backward method of multivariable logistic regression analysis. The discrimination power of the new clinical tool for diagnosis of AIS was assessed with the area under the receiver operating characteristic curve (AUC-ROC). <b>Results:</b> Data from 806 patients were analyzed; of them, 57.4% were men. The mean age of the study patients was 66.9 years [standard deviation (SD) = 13.9]. In the multivariable model, 8 items remained. The AUC-ROC of the new clinical tool was 0.893 [95% confidence interval (CI): 0.869-0.917], and its best cut-off point was score ≥ 3 for positive AIS. At this cut-off point, sensitivity and specificity were 84.42% and 79.72%, respectively. <b>Conclusion:</b> We introduced a new nomogram-based clinical tool for the diagnosis of AIS in the prehospital stage, which has acceptable specificity and sensitivity; moreover, it is comparable with previous tools.</p>\",\"PeriodicalId\":40077,\"journal\":{\"name\":\"Current Journal of Neurology\",\"volume\":\"22 1\",\"pages\":\"58-62\"},\"PeriodicalIF\":0.5000,\"publicationDate\":\"2023-01-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10444598/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Journal of Neurology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.18502/cjn.v22i1.12618\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Journal of Neurology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/cjn.v22i1.12618","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
A nomogram-based clinical tool for acute ischemic stroke screening in prehospital setting.
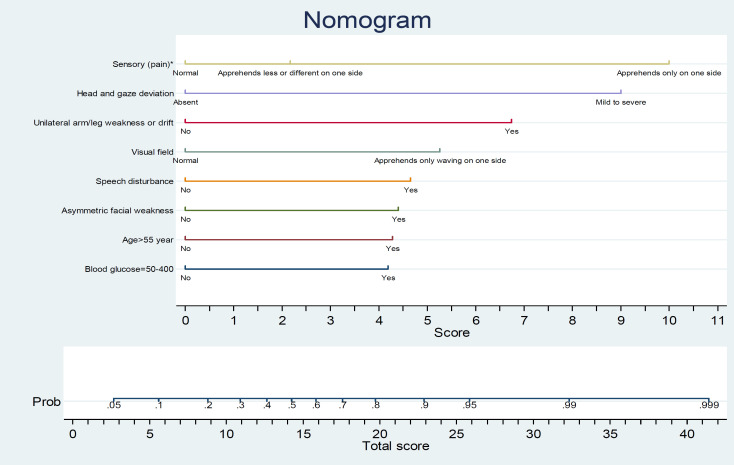
Background: We believe that designing a new tool which is comparable in terms of both sensitivity and specificity may play an important role in rapid and more accurate diagnosis of acute ischemic stroke (AIS) in prehospital stage. Therefore, we intended to develop a new clinical tool for the diagnosis of AIS in the prehospital stage. Methods: This was a cross-sectional diagnostic accuracy study. All patients transferred to the emergency department (ED) who underwent brain magnetic resonance imaging (MRI) with impression of AIS were evaluated by 9 clinical tools for stroke diagnosis in the pre-hospital phase including Rapid Arterial Occlusion Evaluation (RACE), Cincinnati Prehospital Stroke Scale (CPSS), Los Angeles Prehospital Stroke Screen (LAPSS), Melbourne Ambulance Stroke Screen (MASS), Medic Prehospital Assessment for Code Stroke (Med PACS), Ontario Prehospital Stroke Screening Tool (OPSS), PreHospital Ambulance Stroke Test (PreHAST), Recognition of Stroke in the Emergency Room (ROSIER), and Face Arm Speech Test (FAST), and totally 19 items were reviewed and recorded. The new clinical tool was developed based on backward method of multivariable logistic regression analysis. The discrimination power of the new clinical tool for diagnosis of AIS was assessed with the area under the receiver operating characteristic curve (AUC-ROC). Results: Data from 806 patients were analyzed; of them, 57.4% were men. The mean age of the study patients was 66.9 years [standard deviation (SD) = 13.9]. In the multivariable model, 8 items remained. The AUC-ROC of the new clinical tool was 0.893 [95% confidence interval (CI): 0.869-0.917], and its best cut-off point was score ≥ 3 for positive AIS. At this cut-off point, sensitivity and specificity were 84.42% and 79.72%, respectively. Conclusion: We introduced a new nomogram-based clinical tool for the diagnosis of AIS in the prehospital stage, which has acceptable specificity and sensitivity; moreover, it is comparable with previous tools.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


