Catherine L. Boereboom, Rachel B. McGuinness, Philip J. J. Herrod, James E. M. Blackwell, Tanvir S. Sian, Hannah Boyd-Carson, John P. Williams, Jonathan N. Lund, Bethan E. Phillips
{"title":"使用快速计时测试来预测手术风险","authors":"Catherine L. Boereboom, Rachel B. McGuinness, Philip J. J. Herrod, James E. M. Blackwell, Tanvir S. Sian, Hannah Boyd-Carson, John P. Williams, Jonathan N. Lund, Bethan E. Phillips","doi":"10.1002/rco2.36","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Cardiorespiratory fitness (CRF) has important implications for post-operative recovery. The timed-up-and-go (TUG) test is a cheap and simple method to assess a patient's functional performance; although how well TUG correlates with results of a cardiopulmonary exercise test (CPET), the gold standard measure of CRF is unknown. Therefore, the aim of this study was to assess the correlation between CPET-derived parameters of CRF and TUG times in a group of older adults.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Ninety-eight independent community dwelling older adults [mean age: 72 years (range: 61–86), mean body mass index: 26.3 ± 3.1 kg/m<sup>2</sup>, 54 male] were recruited to this study; completing 180 CPET and TUG testing sessions over a 28 month period. The correlation between CPET-derived CRF parameters and TUG time was assessed, and receiver operating characteristic curve analysis was performed to determine clinically useful cut-off points in TUG time.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Median TUG time was 7.1 s [interquartile range (IQR): 4–8.5], median VO<sub>2</sub> peak was 24.4 mL/kg/min (IQR: 20.2–29.2), and the median anaerobic threshold (AT) was 13.4 mL/kg/min (IQR: 8.6–16.5). There was a statistically significant negative correlation between TUG time and AT (<i>r</i> = −0.317, <i>P</i> = <0.0001) and TUG time and VO<sub>2</sub> peak (<i>r</i> = −0.4247, <i>P</i> < 0.0001). Receiver operating characteristic curve analysis determined a TUG time of ≥6.5 s to have an 82% sensitivity and 60% specificity to detect an AT <11.0 mL/kg/min, the point at below which perioperative mortality is known to increase.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Despite strong evidence for the utility of pre-operative CPET in stratifying surgical risk, CPET is not universally available. Our finding of a correlation between TUG time and CPET-derived parameters of CRF (AT/VO<sub>2</sub> peak) suggests that TUG may be a useful surrogate in the pre-operative setting.</p>\n </section>\n </div>","PeriodicalId":73544,"journal":{"name":"JCSM rapid communications","volume":"4 2","pages":"159-165"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/rco2.36","citationCount":"2","resultStr":"{\"title\":\"Using a quick timed-up-and-go test to predict surgical risk\",\"authors\":\"Catherine L. Boereboom, Rachel B. McGuinness, Philip J. J. Herrod, James E. M. Blackwell, Tanvir S. Sian, Hannah Boyd-Carson, John P. Williams, Jonathan N. Lund, Bethan E. Phillips\",\"doi\":\"10.1002/rco2.36\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Cardiorespiratory fitness (CRF) has important implications for post-operative recovery. The timed-up-and-go (TUG) test is a cheap and simple method to assess a patient's functional performance; although how well TUG correlates with results of a cardiopulmonary exercise test (CPET), the gold standard measure of CRF is unknown. Therefore, the aim of this study was to assess the correlation between CPET-derived parameters of CRF and TUG times in a group of older adults.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Ninety-eight independent community dwelling older adults [mean age: 72 years (range: 61–86), mean body mass index: 26.3 ± 3.1 kg/m<sup>2</sup>, 54 male] were recruited to this study; completing 180 CPET and TUG testing sessions over a 28 month period. The correlation between CPET-derived CRF parameters and TUG time was assessed, and receiver operating characteristic curve analysis was performed to determine clinically useful cut-off points in TUG time.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Median TUG time was 7.1 s [interquartile range (IQR): 4–8.5], median VO<sub>2</sub> peak was 24.4 mL/kg/min (IQR: 20.2–29.2), and the median anaerobic threshold (AT) was 13.4 mL/kg/min (IQR: 8.6–16.5). There was a statistically significant negative correlation between TUG time and AT (<i>r</i> = −0.317, <i>P</i> = <0.0001) and TUG time and VO<sub>2</sub> peak (<i>r</i> = −0.4247, <i>P</i> < 0.0001). Receiver operating characteristic curve analysis determined a TUG time of ≥6.5 s to have an 82% sensitivity and 60% specificity to detect an AT <11.0 mL/kg/min, the point at below which perioperative mortality is known to increase.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Despite strong evidence for the utility of pre-operative CPET in stratifying surgical risk, CPET is not universally available. Our finding of a correlation between TUG time and CPET-derived parameters of CRF (AT/VO<sub>2</sub> peak) suggests that TUG may be a useful surrogate in the pre-operative setting.</p>\\n </section>\\n </div>\",\"PeriodicalId\":73544,\"journal\":{\"name\":\"JCSM rapid communications\",\"volume\":\"4 2\",\"pages\":\"159-165\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-03-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1002/rco2.36\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JCSM rapid communications\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/rco2.36\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCSM rapid communications","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/rco2.36","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Using a quick timed-up-and-go test to predict surgical risk
Background
Cardiorespiratory fitness (CRF) has important implications for post-operative recovery. The timed-up-and-go (TUG) test is a cheap and simple method to assess a patient's functional performance; although how well TUG correlates with results of a cardiopulmonary exercise test (CPET), the gold standard measure of CRF is unknown. Therefore, the aim of this study was to assess the correlation between CPET-derived parameters of CRF and TUG times in a group of older adults.
Methods
Ninety-eight independent community dwelling older adults [mean age: 72 years (range: 61–86), mean body mass index: 26.3 ± 3.1 kg/m2, 54 male] were recruited to this study; completing 180 CPET and TUG testing sessions over a 28 month period. The correlation between CPET-derived CRF parameters and TUG time was assessed, and receiver operating characteristic curve analysis was performed to determine clinically useful cut-off points in TUG time.
Results
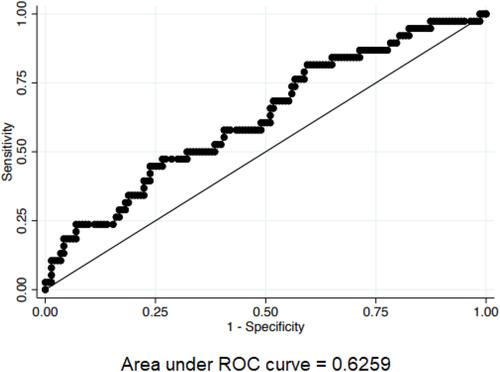
Median TUG time was 7.1 s [interquartile range (IQR): 4–8.5], median VO2 peak was 24.4 mL/kg/min (IQR: 20.2–29.2), and the median anaerobic threshold (AT) was 13.4 mL/kg/min (IQR: 8.6–16.5). There was a statistically significant negative correlation between TUG time and AT (r = −0.317, P = <0.0001) and TUG time and VO2 peak (r = −0.4247, P < 0.0001). Receiver operating characteristic curve analysis determined a TUG time of ≥6.5 s to have an 82% sensitivity and 60% specificity to detect an AT <11.0 mL/kg/min, the point at below which perioperative mortality is known to increase.
Conclusions
Despite strong evidence for the utility of pre-operative CPET in stratifying surgical risk, CPET is not universally available. Our finding of a correlation between TUG time and CPET-derived parameters of CRF (AT/VO2 peak) suggests that TUG may be a useful surrogate in the pre-operative setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


