{"title":"评价单侧和双侧下斜肌切除术对原发性和继发性下斜肌过度活动眼底扭转的影响。","authors":"Omer Faruk Yilmaz, Halit Oguz","doi":"10.14744/nci.2023.74875","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This article evaluates the effects of unilateral and bilateral inferior oblique myectomy (IOM) on fundus torsion in primary and secondary inferior oblique overaction (IOOA).</p><p><strong>Methods: </strong>This study analyzed 230 OCT images of 53 eyes of 32 patients who had undergone IOM by a single surgeon in the last two years. The disc-foveal angle (DFA) was calculated by digitally measuring the angle between the horizontal line passing through the geometric center of the optic disc and the curved line connecting the fovea to the geometric center of the optic disc. DFA was classified into intorsion, normal torsion, and extortion. The DFA was measured from the OCT images before the operation in the first week, first month, third month, and sixth month.</p><p><strong>Results: </strong>When all the patients in our study were evaluated together, IOM statistically reduced the mean DFA in the third month (p=0.00). The DFA was higher in the secondary IOOA group than in the primary IOOA group (p=0.24). Bilateral IOM statistically significantly reduced DFA in the third month (p=0.00) and decreased the DFA difference between the two eyes in the third month (p=0.583). Unilateral IOM increased the DFA, rather than decreasing it, in the first week in operated eyes (p=0594) and increased the DFA difference between the two eyes after surgery (p=0.477). When we evaluated the localization of the macula as an intorsion, normal intorsion, or extortion, the extortion decreased from 36 to nine in the third month after bilateral IOM, and intorsion was seen in only two. Unilateral surgery did not significantly change fundus torsion in primary IOOA, and it caused intorsion in 3 of 6 (50%) operated eyes in secondary IOOA.</p><p><strong>Conclusion: </strong>Although unilateral IOM provides a clinical improvement in secondary IOOA, it increases the difference in DFA between both eyes and causes intorsion in 50% of patients. Masked IOOA was detected in 3 of 11 (27.3%) patients who underwent unilateral IOM. When deciding on unilateral surgery, the possibility of increased DFA difference between both eyes, intorsion in the operated eye, and masked IOOA in the other eye should be considered.</p>","PeriodicalId":94347,"journal":{"name":"Northern clinics of Istanbul","volume":"10 5","pages":"657-665"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/b8/NCI-10-657.PMC10565743.pdf","citationCount":"0","resultStr":"{\"title\":\"Evaluation of the effect of unilateral and bilateral inferior oblique myectomy on fundus torsion in primary and secondary inferior oblique overaction.\",\"authors\":\"Omer Faruk Yilmaz, Halit Oguz\",\"doi\":\"10.14744/nci.2023.74875\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This article evaluates the effects of unilateral and bilateral inferior oblique myectomy (IOM) on fundus torsion in primary and secondary inferior oblique overaction (IOOA).</p><p><strong>Methods: </strong>This study analyzed 230 OCT images of 53 eyes of 32 patients who had undergone IOM by a single surgeon in the last two years. The disc-foveal angle (DFA) was calculated by digitally measuring the angle between the horizontal line passing through the geometric center of the optic disc and the curved line connecting the fovea to the geometric center of the optic disc. DFA was classified into intorsion, normal torsion, and extortion. The DFA was measured from the OCT images before the operation in the first week, first month, third month, and sixth month.</p><p><strong>Results: </strong>When all the patients in our study were evaluated together, IOM statistically reduced the mean DFA in the third month (p=0.00). The DFA was higher in the secondary IOOA group than in the primary IOOA group (p=0.24). Bilateral IOM statistically significantly reduced DFA in the third month (p=0.00) and decreased the DFA difference between the two eyes in the third month (p=0.583). Unilateral IOM increased the DFA, rather than decreasing it, in the first week in operated eyes (p=0594) and increased the DFA difference between the two eyes after surgery (p=0.477). When we evaluated the localization of the macula as an intorsion, normal intorsion, or extortion, the extortion decreased from 36 to nine in the third month after bilateral IOM, and intorsion was seen in only two. Unilateral surgery did not significantly change fundus torsion in primary IOOA, and it caused intorsion in 3 of 6 (50%) operated eyes in secondary IOOA.</p><p><strong>Conclusion: </strong>Although unilateral IOM provides a clinical improvement in secondary IOOA, it increases the difference in DFA between both eyes and causes intorsion in 50% of patients. Masked IOOA was detected in 3 of 11 (27.3%) patients who underwent unilateral IOM. When deciding on unilateral surgery, the possibility of increased DFA difference between both eyes, intorsion in the operated eye, and masked IOOA in the other eye should be considered.</p>\",\"PeriodicalId\":94347,\"journal\":{\"name\":\"Northern clinics of Istanbul\",\"volume\":\"10 5\",\"pages\":\"657-665\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/b8/NCI-10-657.PMC10565743.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Northern clinics of Istanbul\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14744/nci.2023.74875\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Northern clinics of Istanbul","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/nci.2023.74875","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Evaluation of the effect of unilateral and bilateral inferior oblique myectomy on fundus torsion in primary and secondary inferior oblique overaction.
Objective: This article evaluates the effects of unilateral and bilateral inferior oblique myectomy (IOM) on fundus torsion in primary and secondary inferior oblique overaction (IOOA).
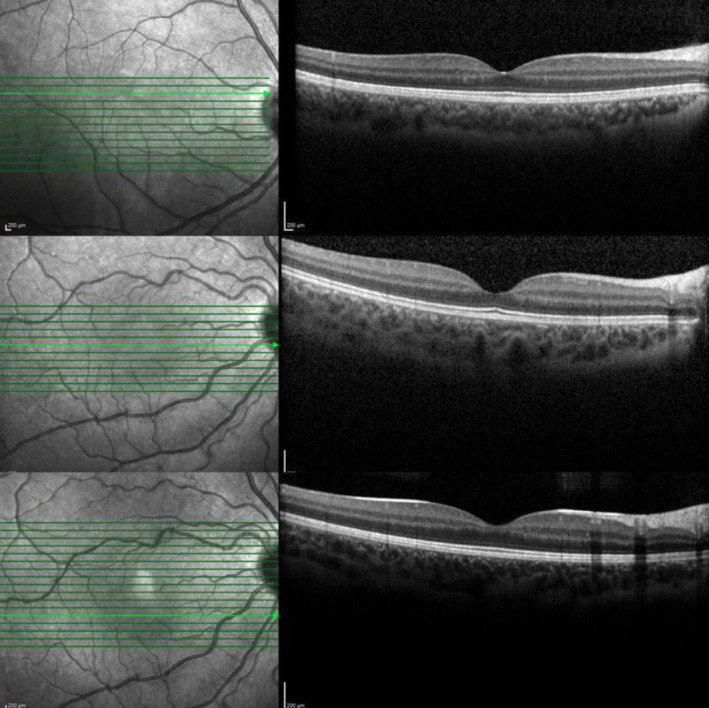
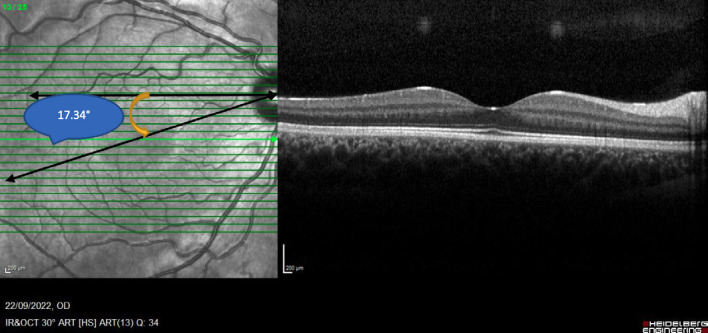
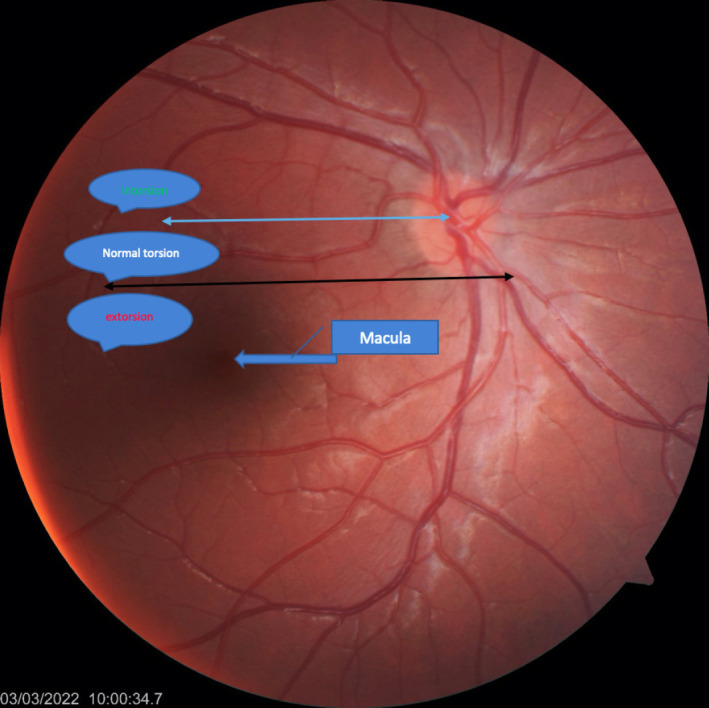
Methods: This study analyzed 230 OCT images of 53 eyes of 32 patients who had undergone IOM by a single surgeon in the last two years. The disc-foveal angle (DFA) was calculated by digitally measuring the angle between the horizontal line passing through the geometric center of the optic disc and the curved line connecting the fovea to the geometric center of the optic disc. DFA was classified into intorsion, normal torsion, and extortion. The DFA was measured from the OCT images before the operation in the first week, first month, third month, and sixth month.
Results: When all the patients in our study were evaluated together, IOM statistically reduced the mean DFA in the third month (p=0.00). The DFA was higher in the secondary IOOA group than in the primary IOOA group (p=0.24). Bilateral IOM statistically significantly reduced DFA in the third month (p=0.00) and decreased the DFA difference between the two eyes in the third month (p=0.583). Unilateral IOM increased the DFA, rather than decreasing it, in the first week in operated eyes (p=0594) and increased the DFA difference between the two eyes after surgery (p=0.477). When we evaluated the localization of the macula as an intorsion, normal intorsion, or extortion, the extortion decreased from 36 to nine in the third month after bilateral IOM, and intorsion was seen in only two. Unilateral surgery did not significantly change fundus torsion in primary IOOA, and it caused intorsion in 3 of 6 (50%) operated eyes in secondary IOOA.
Conclusion: Although unilateral IOM provides a clinical improvement in secondary IOOA, it increases the difference in DFA between both eyes and causes intorsion in 50% of patients. Masked IOOA was detected in 3 of 11 (27.3%) patients who underwent unilateral IOM. When deciding on unilateral surgery, the possibility of increased DFA difference between both eyes, intorsion in the operated eye, and masked IOOA in the other eye should be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


