Hui Lin, Frank Geurts, Luise Hassler, Daniel Batlle, Katrina M Mirabito Colafella, Kate M Denton, Jia L Zhuo, Xiao C Li, Nirupama Ramkumar, Masahiro Koizumi, Taiji Matsusaka, Akira Nishiyama, Martin J Hoogduijn, Ewout J Hoorn, A H Jan Danser
{"title":"心血管疾病中的肾脏血管紧张素:形成和药物靶向。","authors":"Hui Lin, Frank Geurts, Luise Hassler, Daniel Batlle, Katrina M Mirabito Colafella, Kate M Denton, Jia L Zhuo, Xiao C Li, Nirupama Ramkumar, Masahiro Koizumi, Taiji Matsusaka, Akira Nishiyama, Martin J Hoogduijn, Ewout J Hoorn, A H Jan Danser","doi":"10.1124/pharmrev.120.000236","DOIUrl":null,"url":null,"abstract":"<p><p>The concept of local formation of angiotensin II in the kidney has changed over the last 10-15 years. Local synthesis of angiotensinogen in the proximal tubule has been proposed, combined with prorenin synthesis in the collecting duct. Binding of prorenin via the so-called (pro)renin receptor has been introduced, as well as megalin-mediated uptake of filtered plasma-derived renin-angiotensin system (RAS) components. Moreover, angiotensin metabolites other than angiotensin II [notably angiotensin-(1-7)] exist, and angiotensins exert their effects via three different receptors, of which angiotensin II type 2 and Mas receptors are considered renoprotective, possibly in a sex-specific manner, whereas angiotensin II type 1 (AT<sub>1</sub>) receptors are believed to be deleterious. Additionally, internalized angiotensin II may stimulate intracellular receptors. Angiotensin-converting enzyme 2 (ACE2) not only generates angiotensin-(1-7) but also acts as coronavirus receptor. Multiple, if not all, cardiovascular diseases involve the kidney RAS, with renal AT<sub>1</sub> receptors often being claimed to exert a crucial role. Urinary RAS component levels, depending on filtration, reabsorption, and local release, are believed to reflect renal RAS activity. Finally, both existing drugs (RAS inhibitors, cyclooxygenase inhibitors) and novel drugs (angiotensin receptor/neprilysin inhibitors, sodium-glucose cotransporter-2 inhibitors, soluble ACE2) affect renal angiotensin formation, thereby displaying cardiovascular efficacy. Particular in the case of the latter three, an important question is to what degree they induce renoprotection (e.g., in a renal RAS-dependent manner). This review provides a unifying view, explaining not only how kidney angiotensin formation occurs and how it is affected by drugs but also why drugs are renoprotective when altering the renal RAS. SIGNIFICANCE STATEMENT: Angiotensin formation in the kidney is widely accepted but little understood, and multiple, often contrasting concepts have been put forward over the last two decades. This paper offers a unifying view, simultaneously explaining how existing and novel drugs exert renoprotection by interfering with kidney angiotensin formation.</p>","PeriodicalId":19780,"journal":{"name":"Pharmacological Reviews","volume":null,"pages":null},"PeriodicalIF":19.3000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9553117/pdf/","citationCount":"0","resultStr":"{\"title\":\"Kidney Angiotensin in Cardiovascular Disease: Formation and Drug Targeting.\",\"authors\":\"Hui Lin, Frank Geurts, Luise Hassler, Daniel Batlle, Katrina M Mirabito Colafella, Kate M Denton, Jia L Zhuo, Xiao C Li, Nirupama Ramkumar, Masahiro Koizumi, Taiji Matsusaka, Akira Nishiyama, Martin J Hoogduijn, Ewout J Hoorn, A H Jan Danser\",\"doi\":\"10.1124/pharmrev.120.000236\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The concept of local formation of angiotensin II in the kidney has changed over the last 10-15 years. Local synthesis of angiotensinogen in the proximal tubule has been proposed, combined with prorenin synthesis in the collecting duct. Binding of prorenin via the so-called (pro)renin receptor has been introduced, as well as megalin-mediated uptake of filtered plasma-derived renin-angiotensin system (RAS) components. Moreover, angiotensin metabolites other than angiotensin II [notably angiotensin-(1-7)] exist, and angiotensins exert their effects via three different receptors, of which angiotensin II type 2 and Mas receptors are considered renoprotective, possibly in a sex-specific manner, whereas angiotensin II type 1 (AT<sub>1</sub>) receptors are believed to be deleterious. Additionally, internalized angiotensin II may stimulate intracellular receptors. Angiotensin-converting enzyme 2 (ACE2) not only generates angiotensin-(1-7) but also acts as coronavirus receptor. Multiple, if not all, cardiovascular diseases involve the kidney RAS, with renal AT<sub>1</sub> receptors often being claimed to exert a crucial role. Urinary RAS component levels, depending on filtration, reabsorption, and local release, are believed to reflect renal RAS activity. Finally, both existing drugs (RAS inhibitors, cyclooxygenase inhibitors) and novel drugs (angiotensin receptor/neprilysin inhibitors, sodium-glucose cotransporter-2 inhibitors, soluble ACE2) affect renal angiotensin formation, thereby displaying cardiovascular efficacy. Particular in the case of the latter three, an important question is to what degree they induce renoprotection (e.g., in a renal RAS-dependent manner). This review provides a unifying view, explaining not only how kidney angiotensin formation occurs and how it is affected by drugs but also why drugs are renoprotective when altering the renal RAS. SIGNIFICANCE STATEMENT: Angiotensin formation in the kidney is widely accepted but little understood, and multiple, often contrasting concepts have been put forward over the last two decades. This paper offers a unifying view, simultaneously explaining how existing and novel drugs exert renoprotection by interfering with kidney angiotensin formation.</p>\",\"PeriodicalId\":19780,\"journal\":{\"name\":\"Pharmacological Reviews\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":19.3000,\"publicationDate\":\"2022-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9553117/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pharmacological Reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1124/pharmrev.120.000236\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacological Reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1124/pharmrev.120.000236","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Kidney Angiotensin in Cardiovascular Disease: Formation and Drug Targeting.
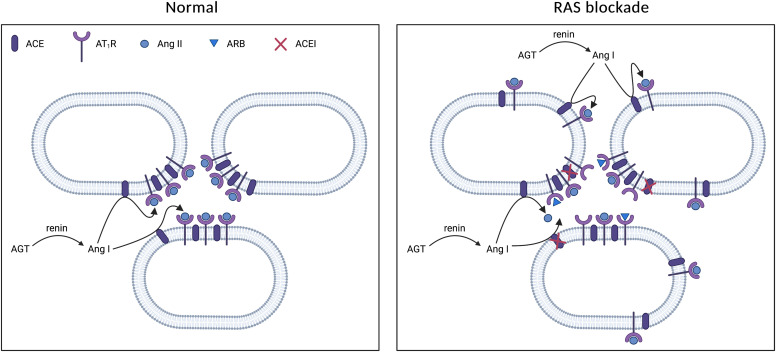
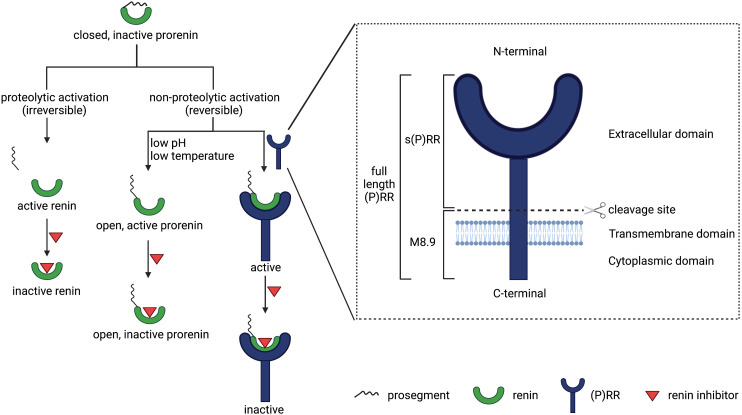
The concept of local formation of angiotensin II in the kidney has changed over the last 10-15 years. Local synthesis of angiotensinogen in the proximal tubule has been proposed, combined with prorenin synthesis in the collecting duct. Binding of prorenin via the so-called (pro)renin receptor has been introduced, as well as megalin-mediated uptake of filtered plasma-derived renin-angiotensin system (RAS) components. Moreover, angiotensin metabolites other than angiotensin II [notably angiotensin-(1-7)] exist, and angiotensins exert their effects via three different receptors, of which angiotensin II type 2 and Mas receptors are considered renoprotective, possibly in a sex-specific manner, whereas angiotensin II type 1 (AT1) receptors are believed to be deleterious. Additionally, internalized angiotensin II may stimulate intracellular receptors. Angiotensin-converting enzyme 2 (ACE2) not only generates angiotensin-(1-7) but also acts as coronavirus receptor. Multiple, if not all, cardiovascular diseases involve the kidney RAS, with renal AT1 receptors often being claimed to exert a crucial role. Urinary RAS component levels, depending on filtration, reabsorption, and local release, are believed to reflect renal RAS activity. Finally, both existing drugs (RAS inhibitors, cyclooxygenase inhibitors) and novel drugs (angiotensin receptor/neprilysin inhibitors, sodium-glucose cotransporter-2 inhibitors, soluble ACE2) affect renal angiotensin formation, thereby displaying cardiovascular efficacy. Particular in the case of the latter three, an important question is to what degree they induce renoprotection (e.g., in a renal RAS-dependent manner). This review provides a unifying view, explaining not only how kidney angiotensin formation occurs and how it is affected by drugs but also why drugs are renoprotective when altering the renal RAS. SIGNIFICANCE STATEMENT: Angiotensin formation in the kidney is widely accepted but little understood, and multiple, often contrasting concepts have been put forward over the last two decades. This paper offers a unifying view, simultaneously explaining how existing and novel drugs exert renoprotection by interfering with kidney angiotensin formation.
期刊介绍:
Pharmacological Reviews is a highly popular and well-received journal that has a long and rich history of success. It was first published in 1949 and is currently published bimonthly online by the American Society for Pharmacology and Experimental Therapeutics. The journal is indexed or abstracted by various databases, including Biological Abstracts, BIOSIS Previews Database, Biosciences Information Service, Current Contents/Life Sciences, EMBASE/Excerpta Medica, Index Medicus, Index to Scientific Reviews, Medical Documentation Service, Reference Update, Research Alerts, Science Citation Index, and SciSearch. Pharmacological Reviews offers comprehensive reviews of new pharmacological fields and is able to stay up-to-date with published content. Overall, it is highly regarded by scholars.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


