Emily Ho, Loris De Cecco, Steven A Eschrich, Stefano Cavalieri, Geoffrey Sedor, Frank Hoebers, Ruud H Brakenhoff, Kathrin Scheckenbach, Tito Poli, Kailin Yang, Jessica A Scarborough, Shivani Nellore, Shauna Campbell, Neil Woody, Tim Chan, Jacob Miller, Natalie Silver, Shlomo Koyfman, James Bates, Jimmy J Caudell, Michael W Kattan, Lisa Licitra, Javier F Torres-Roca, Jacob G Scott
{"title":"包括GARD在内的临床遗传学模型可预测放射治疗的HPV+口咽鳞状细胞癌患者的预后。","authors":"Emily Ho, Loris De Cecco, Steven A Eschrich, Stefano Cavalieri, Geoffrey Sedor, Frank Hoebers, Ruud H Brakenhoff, Kathrin Scheckenbach, Tito Poli, Kailin Yang, Jessica A Scarborough, Shivani Nellore, Shauna Campbell, Neil Woody, Tim Chan, Jacob Miller, Natalie Silver, Shlomo Koyfman, James Bates, Jimmy J Caudell, Michael W Kattan, Lisa Licitra, Javier F Torres-Roca, Jacob G Scott","doi":"10.1101/2023.09.14.23295538","DOIUrl":null,"url":null,"abstract":"<p><p>A central clinical goal for patients with HPV-positive oropharynx cancer has been to reduce radiation doses while maintaining cure rates. Recent results of Phase 3 prospective trial HN005 demonstrated that RT dose de-escalation can not be safely done based on clinical factors alone. We have previously shown that the genomic adjusted radiation dose (GARD) is predictive of radiation treatment benefit and can be used to guide RT dose selection. We hypothesize that GARD can be used to guide RT dose de-escalation in HPV-positive OPSCC patients. Gene expression was analyzed for 191 formalin-fixed paraffin-embedded samples from HPV-positive OPSCC patients within an international, multi-institutional, prospective/retrospective observational study including patients with AJCC 8th edition stage I-III. Two RT dose fractionations were utilized for the majority of primary RT cases (70 Gy in 35 fractions or 69.96 Gy in 33 fractions). Median RT dose was 70 Gy (range 51.0-74.0), survival at 36 months and 60 months was 94.1% and 87.3%, respectively. Cox proportional hazards analyses were performed with GARD as a continuous variable and time-dependent ROC analyses compared the performance of GARD to clinical variables alone. Despite near-uniform RT dosing, GARD reveals significant heterogeneity (range 15.4 - 71.7) in predicted effect. In univariate analysis, GARD was associated with an improvement in OS (HR = 0.941 (0.888, 0.998), p = 0.041). In multivariable analysis, each unit increase in GARD was associated with an improvement in OS (HR = 0.943 (0.891, 0.999), p = 0.046) where stage was not (T stage HR = 1.992 (0.711-5.576), p=0.190, N stage HR = 2.367 (0.867-6.460), p=0.093). ROC analysis for GARD at 36 months yielded an AUC of 78.26 (65.14, 91.38) compared with 71.20 (54.47, 87.93) for standard clinical variables. We identify two GARD-based strategies to RT dose personalization which are predicted to yield improved clinical outcomes, while delivering an average lower RT dose. In this multi-institutional cohort of patients with HPV-positive OPSCC, GARD associates with OS, outperforms standard clinical variables and provides a novel genomic strategy to RT dose personalization. We propose that GARD should be incorporated in the diagnostic workup of HPV-positive OPSCC patients.</p>","PeriodicalId":18659,"journal":{"name":"medRxiv : the preprint server for health sciences","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/41/6e/nihpp-2023.09.14.23295538v1.PMC10516067.pdf","citationCount":"0","resultStr":"{\"title\":\"Personalization of Radiotherapy Dose in HPV Positive Oropharynx Cancer Using GARD.\",\"authors\":\"Emily Ho, Loris De Cecco, Steven A Eschrich, Stefano Cavalieri, Geoffrey Sedor, Frank Hoebers, Ruud H Brakenhoff, Kathrin Scheckenbach, Tito Poli, Kailin Yang, Jessica A Scarborough, Shivani Nellore, Shauna Campbell, Neil Woody, Tim Chan, Jacob Miller, Natalie Silver, Shlomo Koyfman, James Bates, Jimmy J Caudell, Michael W Kattan, Lisa Licitra, Javier F Torres-Roca, Jacob G Scott\",\"doi\":\"10.1101/2023.09.14.23295538\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A central clinical goal for patients with HPV-positive oropharynx cancer has been to reduce radiation doses while maintaining cure rates. Recent results of Phase 3 prospective trial HN005 demonstrated that RT dose de-escalation can not be safely done based on clinical factors alone. We have previously shown that the genomic adjusted radiation dose (GARD) is predictive of radiation treatment benefit and can be used to guide RT dose selection. We hypothesize that GARD can be used to guide RT dose de-escalation in HPV-positive OPSCC patients. Gene expression was analyzed for 191 formalin-fixed paraffin-embedded samples from HPV-positive OPSCC patients within an international, multi-institutional, prospective/retrospective observational study including patients with AJCC 8th edition stage I-III. Two RT dose fractionations were utilized for the majority of primary RT cases (70 Gy in 35 fractions or 69.96 Gy in 33 fractions). Median RT dose was 70 Gy (range 51.0-74.0), survival at 36 months and 60 months was 94.1% and 87.3%, respectively. Cox proportional hazards analyses were performed with GARD as a continuous variable and time-dependent ROC analyses compared the performance of GARD to clinical variables alone. Despite near-uniform RT dosing, GARD reveals significant heterogeneity (range 15.4 - 71.7) in predicted effect. In univariate analysis, GARD was associated with an improvement in OS (HR = 0.941 (0.888, 0.998), p = 0.041). In multivariable analysis, each unit increase in GARD was associated with an improvement in OS (HR = 0.943 (0.891, 0.999), p = 0.046) where stage was not (T stage HR = 1.992 (0.711-5.576), p=0.190, N stage HR = 2.367 (0.867-6.460), p=0.093). ROC analysis for GARD at 36 months yielded an AUC of 78.26 (65.14, 91.38) compared with 71.20 (54.47, 87.93) for standard clinical variables. We identify two GARD-based strategies to RT dose personalization which are predicted to yield improved clinical outcomes, while delivering an average lower RT dose. In this multi-institutional cohort of patients with HPV-positive OPSCC, GARD associates with OS, outperforms standard clinical variables and provides a novel genomic strategy to RT dose personalization. We propose that GARD should be incorporated in the diagnostic workup of HPV-positive OPSCC patients.</p>\",\"PeriodicalId\":18659,\"journal\":{\"name\":\"medRxiv : the preprint server for health sciences\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/41/6e/nihpp-2023.09.14.23295538v1.PMC10516067.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"medRxiv : the preprint server for health sciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1101/2023.09.14.23295538\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"medRxiv : the preprint server for health sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1101/2023.09.14.23295538","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Personalization of Radiotherapy Dose in HPV Positive Oropharynx Cancer Using GARD.
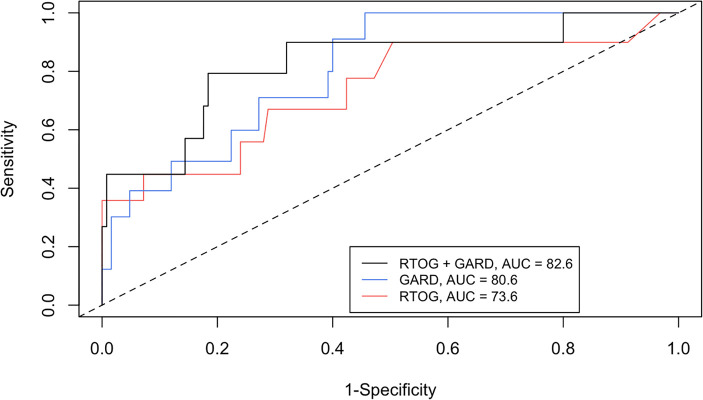
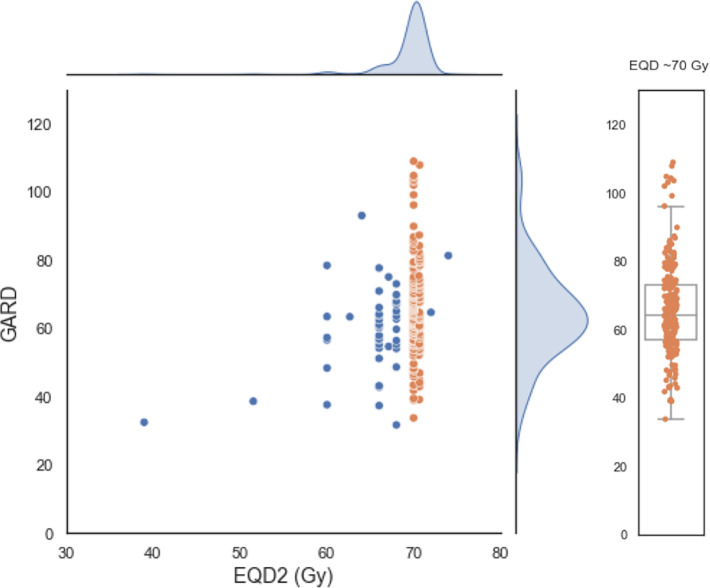
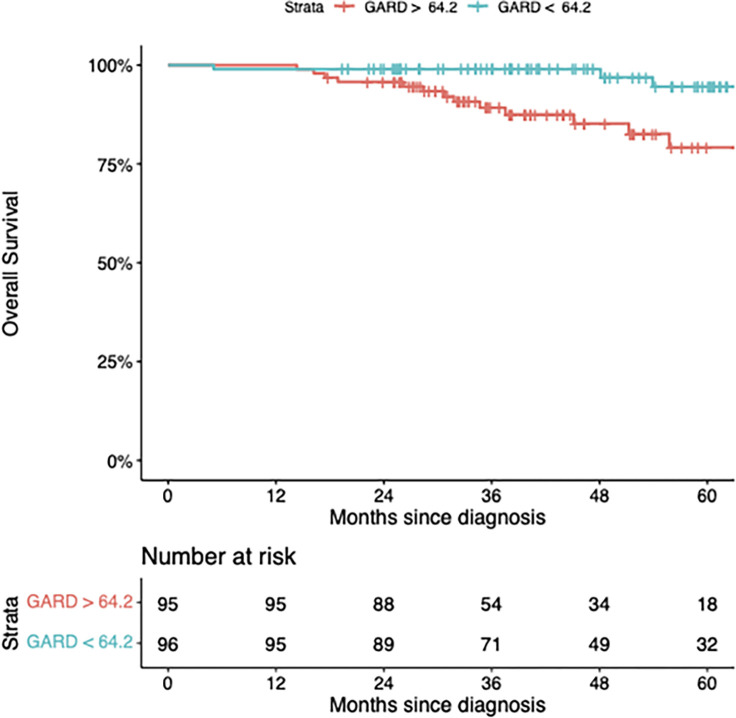
A central clinical goal for patients with HPV-positive oropharynx cancer has been to reduce radiation doses while maintaining cure rates. Recent results of Phase 3 prospective trial HN005 demonstrated that RT dose de-escalation can not be safely done based on clinical factors alone. We have previously shown that the genomic adjusted radiation dose (GARD) is predictive of radiation treatment benefit and can be used to guide RT dose selection. We hypothesize that GARD can be used to guide RT dose de-escalation in HPV-positive OPSCC patients. Gene expression was analyzed for 191 formalin-fixed paraffin-embedded samples from HPV-positive OPSCC patients within an international, multi-institutional, prospective/retrospective observational study including patients with AJCC 8th edition stage I-III. Two RT dose fractionations were utilized for the majority of primary RT cases (70 Gy in 35 fractions or 69.96 Gy in 33 fractions). Median RT dose was 70 Gy (range 51.0-74.0), survival at 36 months and 60 months was 94.1% and 87.3%, respectively. Cox proportional hazards analyses were performed with GARD as a continuous variable and time-dependent ROC analyses compared the performance of GARD to clinical variables alone. Despite near-uniform RT dosing, GARD reveals significant heterogeneity (range 15.4 - 71.7) in predicted effect. In univariate analysis, GARD was associated with an improvement in OS (HR = 0.941 (0.888, 0.998), p = 0.041). In multivariable analysis, each unit increase in GARD was associated with an improvement in OS (HR = 0.943 (0.891, 0.999), p = 0.046) where stage was not (T stage HR = 1.992 (0.711-5.576), p=0.190, N stage HR = 2.367 (0.867-6.460), p=0.093). ROC analysis for GARD at 36 months yielded an AUC of 78.26 (65.14, 91.38) compared with 71.20 (54.47, 87.93) for standard clinical variables. We identify two GARD-based strategies to RT dose personalization which are predicted to yield improved clinical outcomes, while delivering an average lower RT dose. In this multi-institutional cohort of patients with HPV-positive OPSCC, GARD associates with OS, outperforms standard clinical variables and provides a novel genomic strategy to RT dose personalization. We propose that GARD should be incorporated in the diagnostic workup of HPV-positive OPSCC patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


